
A Highly Gifted Juice
Opening Pressure in CSF Analysis and its Role in Idiopathic Intracranial Hypertension
By: Danielle Miller
Case
A 27 year-old obese female with a past medical history of migraines presents with the worst headache of her life.
• The headache was gradual in onset.
• She denies visual changes, tinnitus, syncope, fever, and extremity weakness.
• A non-contrast head CT shows no mass and no blood.
• An LP is performed to rule out SAH and to measure opening pressures.
o Initial opening pressure is 44.
o Closing pressure is 21.
o CSF is negative for blood.
• Patient is admitted for MRI and pain control with presumed diagnosis of idiopathic intracranial hypertension
What is the history behind obtaining opening pressures?
Cerebrospinal fluid was originally identified by Swedish mystic Emanuel Swedenborg in 1736, who described the fluid as a “spirituous lymph’ and “highly gifted juice.”
The first LP was performed in the late 19th century by Heinrich Iraneus Quincke and Walter Essex Wynterin. At that time, there was a high mortality rate of the procedure as the procedure was performed on sick patients and the procedure involved a large incision with a scalpel down to the spinal cord. As early as the 20th century, scientists started to measure opening
Does positioning matter?

Swedish mystic Emanuel Swedenborg
Seriously, leg extension?
Studies suggest that hip flexion may increase CSF opening pressure by increasing intra-abdominal pressure. [5] A study in 1991 found that a flexed position increased opening pressures by 6–8 cm H2O. [6] However, a more recent study in 2001, found differences of only 1–2 cm H2O. [7]
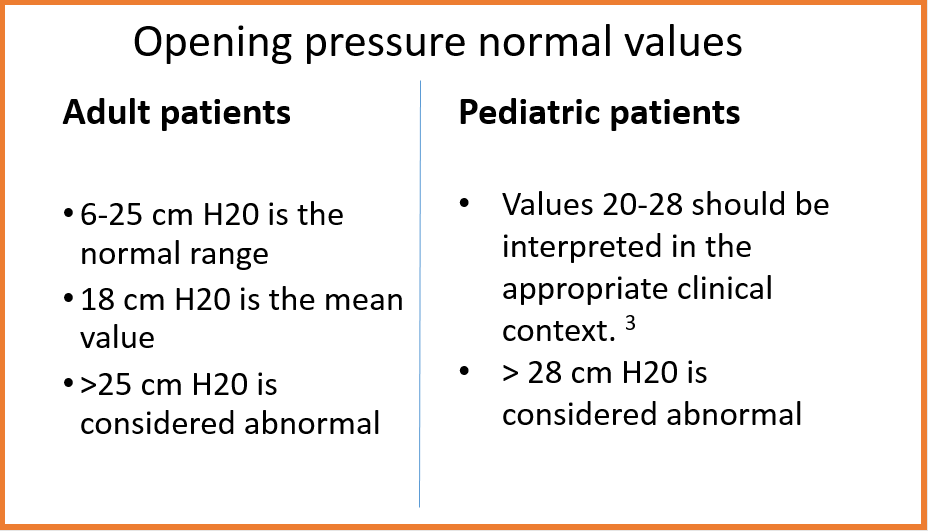
Yes, the patient must be lying in lateral decubitus to essentially zero the manometer. The head should be in line with the right atrium, which should be in line with the spinal needle. The legs should be extended to minimize falsely elevated values. Opening pressures in the seated position are elevated by approximately 25 cm H20. [3]
Does BMI affect opening pressures?

Yes, there is a correlation between BMI and opening pressure, but the values are clinically insignificant, with ranges still remaining 10 cm H20 to 25 cm H20. [8]
What disease states have high opening pressures?
Any process that blocks CSF reabsorption by the arachnoid granulations or increases/obstructs the venous outflow pathway can cause elevated opening pressures, such as:
• Idiopathic intracranial hypertension (IIH)
• Cerebral venous sinus thrombosis
• Intracranial or spinal mass
• Scarring inflammation (sequelae of meningitis, SAH)
Any process that increase venous pressures can also elevate opening pressure, such as:
• Arteriovenous malformations
• Superior vena cava syndrome
• Elevated right heart pressures
Other causes include:
• Hypervitaminosis A
• Addison’s Disease
• Hypoparathyroidism
• Various medications including antibiotics (tetracyclines, nitrofurantoin, and nalidixic acid), amiodarone, cyclosporin, systemic and topical steroids).
Do you need a high opening pressure to diagnose IIH?

Yes and no, IIH is diagnosed with the Dandy criteria:
• Symptoms/signs of increased intracranial pressure such as headache, visual changes.
• No other neurologic deficits or impaired consciousness.
• Elevated intracranial pressure with normal CSF analysis.
• A neuroimaging study that shows no etiology for intracranial hypertension.
• No other cause of intracranial hypertension apparent. [4]
However, if a patient does not have an elevated opening pressure, the patient can still have IIH, given that ICP fluctuates throughout the day. [9]
Why is opening pressure high in IIH?
The true pathophysiology is unknown. Recent studies have suggested that cerebral venous outflow abnormalities lead to elevated intracranial venous pressures, which leads to increased ICP, and thus higher opening pressures. Causes of outflow abnormalities include venous stenosis or venous hypertension. However, none of the studies can determine if the venous abnormalities are the cause of IIH or merely secondary to the disease process itself. [11]
So will the LP that was just performed in the ED on the patient with suspected IIH really alleviate the patient’s headache?
Maybe. Use of LP in symptom management is controversial. CSF returns to pre-tap levels in approximately 82 minutes. Thus, the LP has a short-lived effect on symptom management. [11] [12]
What are treatment options for patients with IIH that present to the ED with headache?
Acetazolamide (Diamox) 250-500 mg BID is recommended and works by decreasing CSF flow. However, because the medication’s effect does not occur until 99.5% of choroid plexus carbonic anhydrase is inhibited, in the acute setting, this may not provide immediate relief. [13]
Furosemide (Lasix) can also treat IIH. Lasix alleviate headache through diuresis and reducing sodium transport into the brain, thus reducing ICP. Outpatient management generally begins at 20 mg BID dosing. [14]
What are the practice patterns for obtaining an opening pressure in the ED?
There is no data on ED practioners’ frequency of obtaining opening pressure as a part of the LP procedure.
Case Conclusion
The patient is admitted to neurology for MRI to exclude secondary causes of increased intracranial pressure. MRI is negative. She returns home with neurology follow-up for likely diagnosis of idiopathic intracranial hypertension.
Take Home Points
Expert Commentary
Great post.
In Emergency Medicine practice, most cases of IIH (pseudotumor cerebri) are diagnosed as described in this case – incidentally. The emergent need for LP is quite rare, focusing on time sensitive conditions (meningitis, subarachnoid hemorrhage). The literature regarding the emergent need for LP to rule out IIH is somewhat unclear. For example, I once had a primary care provider send a patient to the ED for “an emergent diagnostic LP to rule out pseudotumor.” His patient presented as an outpatient with blurred vision, a new gradual onset headache, and had recently started an anti-acne medication containing Vitamin A (OCP’s, Vitamin A, tetracycline, and thyroid disorders can all cause IIH). The data / reasoning behind sending this patient to the ER for an emergent LP is murky at best. Could the primary care provider simply have dilated the eyes and look for papilledema? Used an ultrasound if he did not trust his exam? Referred the patient urgently to IR or neurology? Many will opt to simply refer the patient to the ED.
One study shows that patients who experience worsening visual field defects despite medical therapy, or have the presence of visual acuity loss attributed to papilledema, do have improvement in vision following surgical therapy (optic nerve sheath fenestration, shunting, venous sinus stenting). Br J Ophthalmol. 2014 Oct;98(10):1360-3. Epub 2014 May 12.
Therefore, it seems reasonable that a patient at high risk for IIH who has new visual acuity or field deficits should receive an urgent or emergent LP in combination with an evaluation for papilledema (dilation or ultrasound) in order to properly expedite further care. The time frame within which this needs to occur (urgent vs emergent) is not currently clear. For my personal practice in the community, if your pre-test probability for IIH is high, and your vision is worsening, you will usually get an LP, unless I can arrange for close specialist re-evaluation within 24 hours.
References
1 Pickover, Clifford. The Medical Book: 250 Milestones in the History of Medicine. New York: Sterling Publishing, 2012. Print.
2 Pearce JM. Walter Essex Wynter, Quincke, and lumbar puncture. J Neurol Neurosurg Psychiatry. 1994;57(2):179.
3 Lee SC1, Lueck CJ. Cerebrospinal fluid pressure in adults. J Neuroophthalmol. 2014 Sep;34(3):278-83.
4 Lee, Andrew and Michael Wall. Idiopathic intracranial hypertension (pseudotumor cerebri): Clinical features and diagnosis. Uptodate. 17 June 2015.
5 Corbett JJ, Mehta MP. Cerebrospinal fluid pressure in normal obese subjects and patients with pseudotumour cerebri. Neurology. 1983;33:1386–1388.
6 Watanabe S, Yamaguchi H, Ishizawa Y. Level of spinal anesthesia can be predicted by the cerebrospinal fluid pressure difference between flull-flexed and non-full-flexed lateral position. Anesth Analg. 1991;73:391–393.
7 Abbrescia KL, Brabson TA, Dalsey WC, Kelly JJ, Kaplan JL, Young TM, Jenkins D, Chu J, Emery MS; Lumbar Puncture Study Group. The effect of lower-extremity position on cerebrospinal fluid pressures. Acad Emerg Med. 2001;8:8–12.
8 Whiteley W1, Al-Shahi R, Warlow CP, Zeidler M, Lueck CJ. CSF opening pressure: reference interval and the effect of body mass index. Neurology. 2006 Nov 14;67(9):1690-1.
9 Wall, Micaheal. Idiopathic Intracranial Hypertension. Neurol Clin. 2010 Aug; 28(3): 593–617.
10 Sharma, Dushyant, et al. "Addison's disease presenting with idiopathic intracranial hypertension in 24-year-old woman: a case report." Journal of medical case reports 4.1 (2010): 60.