


Written by: Gabby Ahlzadeh, MD (NUEM PGY-4) Edited by: Rachel Haney, MD (NUEM Alum '17) Expert commentary by: Gentry Wilkerson, MD (University of Maryland)
It’s a busy overnight and the nurses are speedily wheeling a gentleman from triage to the resuscitation bay. “It’s an allergic reaction, come quick!” You take a look at the patient: no respiratory distress, no lip swelling, no facial swelling, no hives, seems pretty comfortable. You ask a question and the patient has a hot potato muffled voice and seems like he has something stuck in the back of his throat. No wheezing, satting well on room air, no trismus, the patient opens wide and all you see is uvula: edematous, enlarged, looks like a very large grape. The patient is tolerating his secretions well otherwise. Is this an allergic reaction w/no other systemic symptoms and no clear precipitant? Is this uvulitis? Is there a peritonsillar abscess? Does this person need to be intubated?
3 recent cases demonstrate the wide variety of ways that uvular edema can present:
Case 1
A male took a few shots of aged whiskey prior to sleeping then woke up a few hours later with a swollen uvula, no other allergic symptoms. He improved with IM epinephrine x3, NP scope showed normal appearing epiglottis and vocal cords; he was admitted to the ICU for close monitoring and had resolution of symptoms within 24 hours.
Case 2
An older gentleman on an ACE-inhibitor presented with 2 weeks of sore throat. He had isolated uvular edema years ago after drinking vodka. He avoided vodka since then, but drank tequila the night prior to presentation and woke up with a grapelike uvula. We treated him for infectious and allergic causes and he was also admitted for respiratory monitoring.
Case 3
A man in town for business who had previously had uvular edema and was usually able to manage his symptoms at home with Benadryl and IM epi, but had forgotten his epi pen in a different suitcase. He improved after steroids, epinephrine, antihistamines. After a period of observation he wanted to leave. We discharged him with steroids and an epi pen and recommended he follow up with an allergist.
Differential for uvular edema:
Epiglottitis – fever, drooling, anxiety, airway obstruction, think of kids, get lateral neck films and be careful examining the kids- they need to be kept calm as agitation can worsen airway obstruction!
Retropharyngeal abscesses or cellulitis – midline or unilateral swelling of posterior oropharynx, stridor tachypnea, won’t extend the neck, fever, intense pain with swallowing, think CT scan
Peritonsillar abscess – tonsillar swelling, deviated uvula, fever, sore throat, trismus, hot potato voice (only 1 case of uvulitis w/PTA has been reported).
Angioedema – AKA Quincke’s edema, foreign body sensation, grape like in appearance, uvular hydrops, maybe eosinophilia on CBC, similar occurrence in the past
Viral exanthem – vesicular lesions
Severe pharyngitis – pharyngeal edema sore throat, palatal petechial, tonsillar enlargement, exudates
Mechanical Trauma – ulceration of the uvula, compression from LMA or ETT, recent ENT procedure
Drugs – inhaled cocaine, cannabis, herbal medicines like the juice of the squirting cucumber or Ecballium elaterium, used as a homeopathic remedy for sinusitis. Can be the exposure itself or as a result of thermal injury.
Hereditary angioneurotic edema (HANE) – autosomal dominant genetic form, lack of C1 esterase inhibitor protein, think about w history of repetitive episodes of uvular edema, family history, confirmed with blood samples showing low C1 esterase levels. If suspected, can use bradykinin receptor antagonist (Icatibant) or complement C1 inhibitor concentrate (Berinert, Cinryze).
Literature:
Most cases are case reports and involve exposure to drugs, inhaled substances.
One Spanish study from 2010 found that of 58 patients who presented with uvular edema, 75.9% presented with isolated uvular edema; 55.1% were idiopathic with predisposing factors of being overweight, longer uvula, GERD, and having a tendency to snore. Recurrent episodes were more common in the idiopathic group as well
Snoring has been found to precipitate uvular angioedema in patients taking ACE inhibitors
While it seems there is no specific data about management of idiopathic cases, most are treated as caused by an allergic reaction
There is no clear cut recommendation about whether these individuals should be admitted for respiratory monitoring or whether isolated uvular edema can truly obstruct the airway
Management:
If infectious etiology (fever, pain), treat as such and the uvular edema is likely reactive. Think group A streptococci, Haemophilus influenzae, Streptococcus pneumoniae
Keep patient in upright position to minimize airway obstruction
Rule out epiglottitis ASAP with lateral neck films or NP scope if patient can tolerate
Allergy cocktail: antihistamine, epinephrine, steroids, H2 blocker; discharge with Epi pen
Uvula irritates posterior OP causing nausea, so Zofran can help
Topical epinephrine or inhaled nebulized epinephrine for vasoconstriction to decrease edema
Needle decompression of uvula has been done in the past with only anecdotal evidence
Rhinolaryngoscopy to rule out epiglottitis if patient is not improving over time; might be a good idea to have the ETT loaded onto the scope just in case there is cord edema or acute airway obstruction during the procedure.
If intubation is needed, the uvula will certainly be in the way so reach for the fiberoptic scope or just clamp the uvula and pull it to the side.
Consider observation for airway monitoring
Expert Commentary
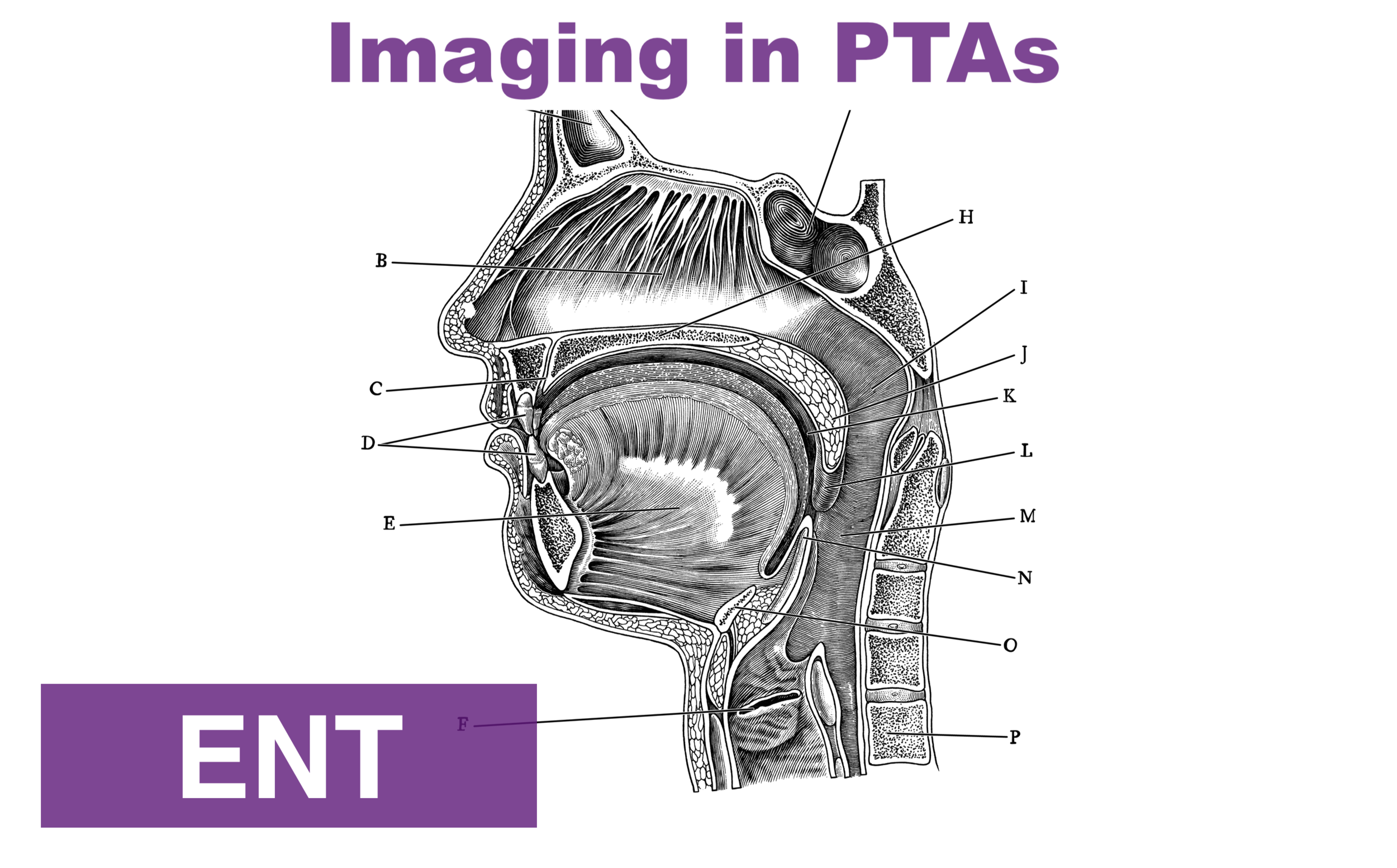
This blog post is an interesting discussion about the patient presenting with isolated uvular swelling. The uvula is the fleshy structure that hangs from the soft palate in the posterior pharynx. It is composed of glandular and connective tissue with interspersed muscle fibers. Seromucous glands within the uvula produce much of the total volume of saliva. Patients presenting with uvular complications will often have some combination of dysphonia, dysphagia, and dyspnea.
The underlying cause of uvular swelling can be due to trauma, infection, inflammation, and angioedema due to allergic reactions and non-allergic mechanisms. Performing a comprehensive history and physical will often help provide guidance about the cause of the problem. However, up to half of all cases of uvular swelling will have no identifiable cause. Trauma to the uvula can occur as a result of direct physical contact, thermal or cold exposure, and vibration (as with snoring). Uvular hematoma has been seen in cases of thrombolytic administration. Isolated infection of the uvula is very uncommon. It usually occurs in the setting of more widespread infection as with pharyngitis, tonsillitis, or epiglottitis. Pathogens responsible include Haemophilus and Streptococcus species as well as due to candidal infections.
Angioedema is a term that describes the physical exam finding of transient, nonpitting swelling of subcutaneous tissue or of the submucosal layer of the respiratory or gastrointestinal tracts. Isolated uvular angioedema has been called Quinke’s edema in recognition of Heinrich Quinke’s contribution to the understanding of angioedema. Most forms of angioedema result from increased levels of either histamine or bradykinin. Histaminergic angioedema is typically allergic or immunologic. Bradykinin-mediated forms of angioedema include hereditary angioedema, acquired angioedema, ACE-inhibitor induced angioedema. The term “angioneurotic edema” is archaic and refers to the earlier belief that angioedema was the result of neurologic or psychiatric disturbances. Differentiating between histaminergic and bradykinin-mediated forms of angioedema can be difficult due to the lack of available testing in the Emergency Department. Histaminergic forms may be associated antecedent exposure to a possible allergen and subsequent development of urticaria and pruritus whereas bradykinin-mediated forms are not.
Regardless of the cause of uvular swelling, the most important component of treatment is airway management. There is no definitive point at which it can be clearly determined that a definitive airway needs to be obtained. The decision must be made based on a combination of factors including rapidity of disease progression, anatomic considerations that may make intubation more difficult and equipment available to the clinician. Once the decision to intubate is made, it should be performed by the most experienced provider with anticipation of a difficult airway. Many experts suggest preparing a “double set-up” where the neck is prepped for a cricothyroidotomy in the event of a failed airway.
Performance of nasopharyngoscopy is somewhat controversial but I believe that it is of great importance to fully understand the extent of disease. The clinician should be aware that any physical manipulation of the airway may result in worsening of the swelling and therefore he or she should be prepared to immediately secure the airway.
Frequently, cases are treated with a shotgun approach where patients are treated with epinephrine, steroids and antihistamines. In cases of hereditary angioedema there are now a number of FDA-approved medications that act by replacing C1 esterase inhibitor (C1-INH), inhibiting kallikrein mediated breakdown of high molecular weight kininogen (HMWK) into bradykinin or inhibiting the bradykinin B2 receptor. Despite case reports and case series none of these have been shown to be effective in ACE inhibitor induced angioedema. Fresh frozen plasma contains both C1-INH and angiotensin converting enzyme (ACE, also known as kininase II), which may help to reduce the swelling associated with bradykinin-mediated forms of angioedema. FFP also contains HMWK and kallikrein, which may result in increased formation of bradykinin. Any concern for infection should prompt the clinician to provide appropriate antimicrobial or antifungal coverage.
Any patient that has swelling involving the airway will need close monitoring until the swelling resolves. Most will require admission to an intensive care unit where prompt airway management can occur in the event of clinical deterioration. In 1999, Ishoo et al performed a single-center, retrospective review of patients admitted over an eleven-year period with angioedema due to all causes. They found the following factors were associated with an increased risk of need for definitive airway: voice change, hoarseness, stridor and dyspnea. Patients were categorized by the location of angioedema into 4 non-continuous stages. Application of this categorization has limitations as there have been numerous advances in management in the two decades since this was published.

Gentry WIlkerson, MD
Assistant Residency Program Director, University of Maryland Medical Center
How to Cite this Post
[Peer-Reviewed, Web Publication] Ahlzadeh G, Haney R (2018, September 3). Uvular Edema. [NUEM Blog. Expert Commentary by Wilkerson G]. Retrieved from http://www.nuemblog.com/blog/uvular-edema
Other Posts You May Enjoy



References:
Alcoceba E, Gonzalez M, Gaig P, et al. Edema of the Uvula: Etiology, Risk Factors, Diagnosis and Treatment. J Investg Allergol Clin Immunol. 2010;20(1):80-3. http://www.jiaci.org/issues/vol20issue1/12.pdf
Evans TC, Roberge RJ: Quincke's disease of the uvula. Am J Emerg Med 1987;5:211-216.
Goldberg R, Lawton R, Newton E et al. Evaluation and management of acute uvular edema. Ann Emerg Med.1993;22:251-255
Kuo DC, Barish RA. Isolated uvular angioedema associated with ace inhibitor use. J Emerg Med 1995;13:327–30
Rasmussen E, Mey K, Bygum A. Isolated oedema of the uvula induced by intense snoring and ACE inhibitor. BMJ Case Reports, vol 2014; 2014.
Roberts J. Acute angioedema of the Uvula. Emergency Medicine News. 2001;23(7):7-12.
Welling A. Enlarged uvula (Quincke’s Oedema) – A side effect of inhale cocaine? – a case study and review of the literature. International Emergency Nursing. 2008;16(3):207-10.