

Author: Andrew Cunningham, MD (EM Resident Physician, PGY-1, NUEM) // Edited by: Logan Weygandt, MD (EM Resident Physician, PGY-3, NUEM)
Citation: [Peer-Reviewed, Web Publication] Cunningham A, Weygandt L (2016, January 12). A Camel Through The Eye Of A Needle. [NUEM Blog. Expert Peer Review by Beach C]. Retrieved from http://www.nuemblog.com/blog/nasal-fiberoptic/
The Patient
Severe tongue angioedema. Image Courtesy of LITFL.
You are just finishing up a tough overnight shift. It is almost time to sign out and head home for some Game of Thrones reruns and well-deserved Z’s. An experienced nurse asks you to take a quick look at room 11. The patient is an elderly male whose chief complaint is tongue itching and swelling, but no difficulty breathing. You see this:
This patient’s airway is not protected. It is time to get a tube in place before the patient decompensates and requires a crash airway. While there are several available options for intubating this patient such as awake- direct or video laryngoscopy, fiber-optic intubation is likely best. Although fiberoptic intubation can be done orally or nasally, the nasal approach is preferred in patients with a large tongue, limited mouth opening, tracheal deviation, or jaw abnormalities [1]. Per Dr. Levitan, “When the mouth is off limits, nasal intubation can be a valuable technique for gaining an emergency airway [2].”
A Step-by-Step Approach to Nasopharyngeal Fiberoptic Intubation
- Ask the patient to occlude each nostril one at a time. Whichever one is easier to breathe through will be the most patent nostril, and your target for this procedure. Alternatively, and less humanely, you may place your lubricated small finger in each of the patient’s nares to determine the larger side.
- If the patient is currently stable, consider first dilating the nostril with a lidocaine jelly-lubricated nasal trumpet. You may also consider using cocaine-soaked cotton-tipped applicators of increasing numbers to serially dilate the nare.
- Administer your choice of local anesthetic: Nebulized 4% lidocaine can be helpful in anesthetizing the entire upper airway, but if time does not permit this, a transoral atomizer or nasal lidojet approach can be effective. You may also spray lidocaine via the side-port on the bronchoscope during passage through the nasopharynx. If time is available, consider agents to decrease secretions such as glycopyrrolate (0.2mg IV) or scopolamine patch.
- Apply vasoconstrictors such as phenylephrine drops or Afrin spray to the nose; this can help limit epistaxis and ensure good visual passage with the bronchoscope.
- When using sedation, simply remember your goal is to limit the patient’s movement, not stop their own spontaneous respirations. There are many available sedation options. Dexmedetomidine may be particularly useful, given that it does not cause respiratory depression and decreases secretions. Also consider the dissociative agent Ketamine.
- Place the well-lubricated tube over the scope, and pass the scope through the nostril OR place the well-lubricated tube in the nostril, advancing to 14-16 cm, and pass the scope through the tube.
- Advance the scope towards the larynx until the vocal cords and epiglottis are visualized.
- If the tongue is in the way, have an assistant either put some gentle traction on the tongue or perform a jaw-lift maneuver.
- Keep advancing the scope to the carina, and pass the tube over it. Make sure to keep the bevel toward the septum as you would with a nasopharyngeal airway [1,3,4,7].
Tube First Versus Scope First
In the above step-by-step description, you will notice there are two different options at step 6: placing the tube first, or placing the scope first. Either method is acceptable, with each one having its own advantages and disadvantages. Here’s a table to help guide your decision:
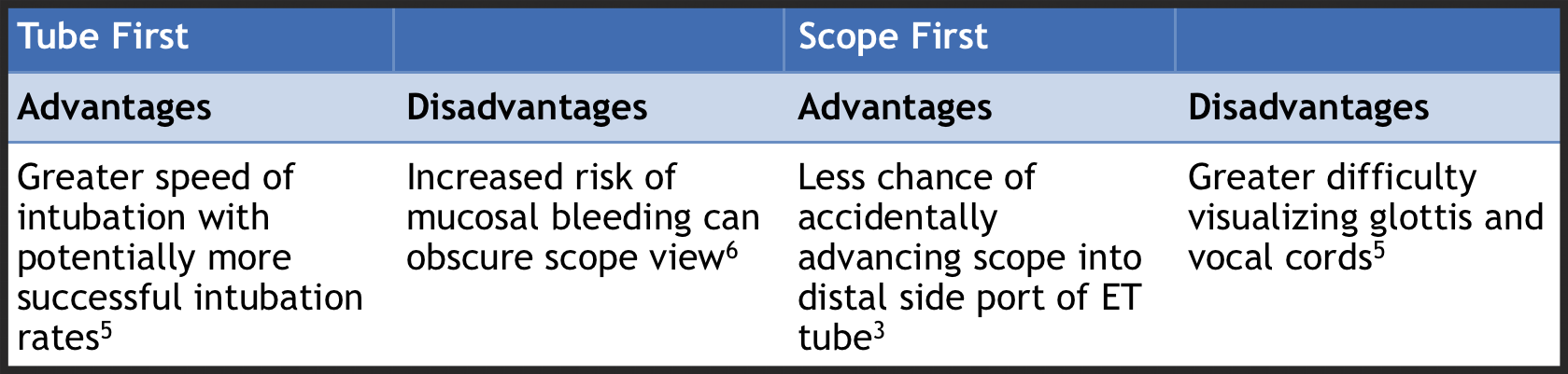
Ultimately, there is no standard of care in regards to technique. A 2011 Iranian study suggests that passing the tube first may lead to greater success rates, but the study did not have enough power to demonstrate a statistically significant benefit to tube-first nasotracheal intubation [5].
Tube First Tips
If choosing to pass the tube first, the physician is faced with the challenge of inserting the tube to an appropriate distance that allows for appropriate visualization of the laryngeal opening after the bronchoscope is passed through the pre-placed tube. A reasonable approach is to insert the tube to approximately 14-16 cm while directing the ETT toward the contralateral nipple. If breath sounds can be heard through the tube, it is likely placed above the laryngeal inlet, and ready for insertion of the bronchoscope. The final ETT length after placement past the cords should be approximately 26 cm and 28 cm at the nose for women and men respectively.
Take-Home Points
- Consider fiberoptic nasopharyngeal intubation in patients with known or anticipated difficult airway.
- Ensure adequate sedation and topicalization of the patient to increase the likelihood of a successful intubation.
- When deciding to place the tube or the scope first, consider the advantages and disadvantages of either approach.
Expert Commentary
This is a nice, concise review of awake nasopharyngeal fiberoptic intubation. Nasal airway approaches have been used for over 100 years. However, higher rates of complications, including bleeding, trauma, sinusitis and failure to secure the airway due to lack of direct visualization have resulted in a preference for oropharyngeal approaches. Nonetheless, it is an alternative (and in some ways – a lost art) useful in situations such as this.
In this scenario – first things first. Don’t panic (others likely will). This glottic swelling didn’t occur in a few seconds, or likely even in a few minutes. Preparation, as listed in steps 1-4 is vital to improving chances at successful management. Medication use is an important component of the next steps and includes such medicines as odansetron (vomiting would result in potential disaster), subcutaneous epinephrine, steroids and H1/H2 blockers. Sedatives are also important as most patients are anxious. Dexmedetomidine was mentioned but other choices are also valuable, such as ketamine or midazolam. Benzodiazepines have the added benefit of antiemetic properties and opiates such as fentanyl, in small doses, help blunt the cough reflex. In any awake airway procedure expect and prepare for both gagging and coughing. In addition to the parenteral medicines described, local anesthetic application whether through nebulization, topical application or injection are beneficial. Local injections may include superior laryngeal nerve or inferior alveolar nerve blocks or direct transtracheal injection.
With either tube first or scope first approach, the steps preceding them (preparation) are still the most critical. Fiberoptic intubation is not a common first choice approach to airway management in ED’s. However, many patients can benefit from this approach, beyond those with critical anatomical concerns. Performing the procedure in stable patients will prepare one well for those rare moments when we are presented with difficult anatomy. In the end, every airway should be approached cognitively as a ‘difficult airway’ and, by doing so, the clinician will be well prepared for whatever comes their way.

Christopher Beach, MD
Vice Chairman and Associate Professor of Emergency Medicine Northwestern University Feinberg School of Medicine – Department of Emergency Medicine; Chief, Northwestern Lake Forest Hospital - Department of Emergency Medicine
References:
- Collins, S. R., and R. S. Blank. 'Fiberoptic Intubation: An Overview And Update'. Respiratory Care 59.6 (2014): 865-880. Web.
- Levitan, R. Nasal Intubation. Emergency Physicians Monthly. 2013. http://epmonthly.com/article/nasal-intubation/. Accessed 11/19/2015.
- Custalow, Catherine B et al. Roberts And Hedges' Clinical Procedures In Emergency Medicine. Philadelphia, PA: Elsevier/Saunders, 2013. Print.
- Dhasmana, Satish Chandra. 'Nasotracheal Fiberoptic Intubation: Patient Comfort, Intubating Conditions And Hemodynamic Stability During Conscious Sedation With Different Doses Of Dexmedetomidine'. Journal of Maxillofacial and Oral Surgery 13.1 (2013): 53-58. Web.
- Mohammadzadeh, Ali et al. 'Comparison Of Two Different Methods Of Fiber-Optic Nasal Intubation: Conventional Method Versus Facilitated Method (NASAL-18)'. Ups J Med Sci 116.2 (2011): 138-141. Web.
- Lee, Jiwon et al. 'Optimal Length Of The Pre-Inserted Tracheal Tube For Excellent View In Nasal Fiberoptic Intubation'. Journal of Anesthesia (2015): n. pag. Web. 5 Nov. 2015.
- Nasal Intubation. Critical Care Compendium. http://lifeinthefastlane.com/ccc/nasal-intubation/. Accessed 11/19/2015.