

Guidance on the use of CT imaging in pediatric patients with head trauma
Posts filed under Pediatrics
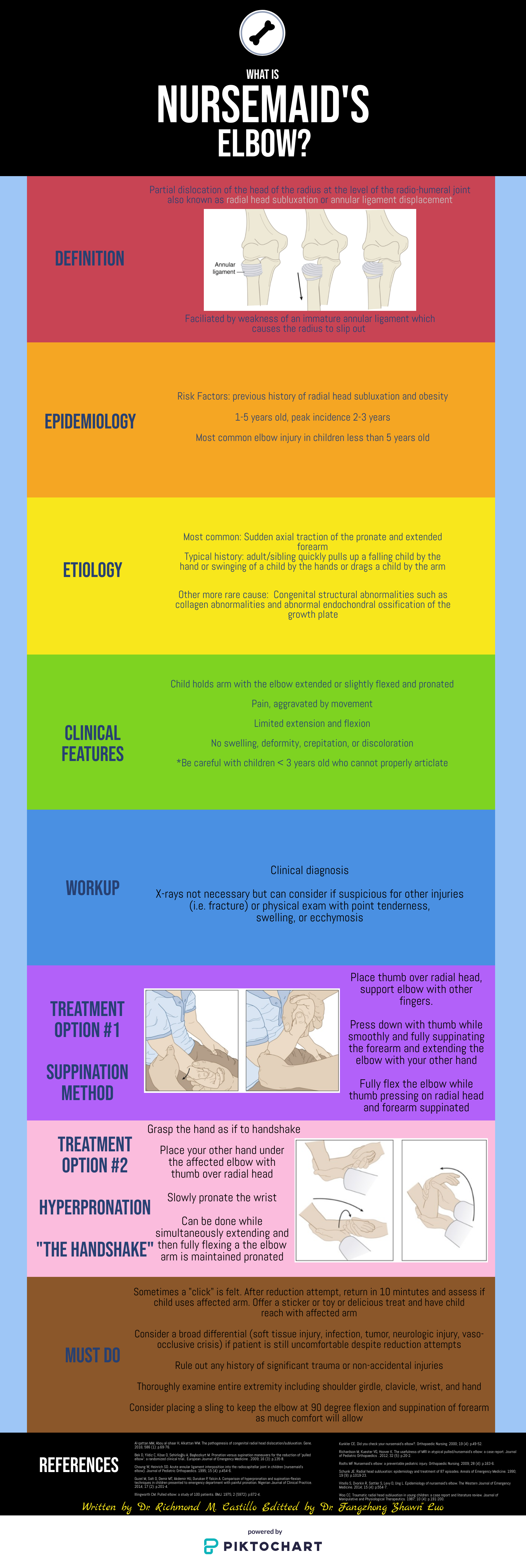
Nursemaid's Elbow

Written by: Richmond Castillo, MD (NUEM ‘23) Edited by: Shawn Luo, MD (NUEM ‘22)
Expert Commentary by: Jacob Stelter, MD (NUEM ‘19)
Expert Commentary
This is an excellent summary of the diagnosis and management of radial head subluxation (nursemaid’s elbow) in children. Clinically, as pointed out, these patients are usually toddlers and will come in after an injury to the arm. Usually, the clinical history will involve the child’s arm having been pulled on while the elbow was extended leading to sudden onset of pain and reduced mobility of the arm. The patient will most often be holding the elbow in flexion and be resistant to having it manipulated. In general, I have a low threshold to obtain radiographs on these patients. If the story and exam is classic for a radial head subluxation, imaging is technically not indicated, and reduction can be attempted. However, more often than not, the history can be vague, and the mechanism of injury may be unclear. In this situation, it is better to rule out a fracture first than to attempt a reduction without imaging. Attempted reduction could worsen or lead to displacement of a supracondylar humerus fracture if that is present. Keep in mind that it is not uncommon for the subluxation to reduce spontaneously during the process of obtaining x-rays.
There are two preferred techniques for reduction of a radial head subluxation. The method I start with is to support the patient's elbow and forearm and gently supinate the forearm while flexing the elbow and applying gentle pressure over the radial head. A “pop” sensation will often be felt as the radial head reduces. The other technique that can be used is to hyper-pronate the forearm while maintaining the elbow in a flexed position. Both of these techniques have a high success rate. Typically, the child will start using the arm again, but it may not be immediate. I will typically reassess the patient about 10-15 minutes post-reduction to ensure they are using their arm normally again. If the child is using their arm and able to extend and flex at the elbow without pain, they can be discharged, and no splinting is necessary. If no radiographs were obtained prior to reduction and the patient is not back to baseline post-reduction, x-rays should be obtained to rule out a fracture. Keep a broad differential, especially if the patient is not responding as you would expect or has other vital sign or exam abnormalities.

Jacob Stelter, MD, CAQ-SM
Division of Emergency Medicine | NorthShore University HealthSystem
NorthShore Orthopaedic Institute | Primary Care Sports Medicine
Clinical Assistant Professor | University of Chicago Pritzker School of Medicine
How To Cite This Post:
[Peer-Reviewed, Web Publication] Castillo, R. Luo, F. (2022, Feb 7). Nursemaid’s Elbow. [NUEM Blog. Expert Commentary by Stelter, J]. Retrieved from http://www.nuemblog.com/blog/nursemaids-elbow.
Other Posts You May Enjoy






Hip Pain in Pediatrics
Written by: Tommy Ng, MD (NUEM ‘24) Edited by: Patricia Bigach, MD (NUEM ‘22) Expert review by: Terese Whipple, MD '20
So your kid won’t walk
One of the most common complaints in a pediatric Emergency Department is a child refusing or inability to ambulate. For normal development, a child is typically able to stand at 9 months, walk at 12 months, and run at 18 months. There is a certain degree of variability for these age constraints however any acute decrease in mobility should prompt an evaluation. A limp is defined as any abnormality in gait caused by pain, weakness, or deformity [1]. There are a plethora of conditions that can manifest with an antalgic gait or refusal to bear weight and it may be difficult to distinguish between etiologies given a child’s age.
History and physical
Age is an important factor as certain conditions are more likely depending on the patient’s age
Acuity should be determined as the chronicity of limp as certain etiologies are more acute while others are indolent. Additionally, certain infectious etiologies are more likely to present acutely or chronically.
Fever may suggest an infectious or rheumatologic cause
Trauma can help distinguish soft tissue vs orthopedic injuries
Past medical history is important to be focused on recent illnesses, antibiotic use, history of sickle cell disease, or hormonal diseases.
Physical examination should always include an attempt to ambulate the child unless there is an obvious contraindication noted immediately (eg open fracture). If the child refuses to bear weight, the child should be made non-weight bearing until serious pathology which can be worsened by walking is ruled out. Strength and range of motion of both lower extremities should also be examined [2].
Normal gait cycle (orthobullets.com)
Differential: the bad, the worse, and the ugly
Infectious
Transient Synovitis - Relatively common with a lifetime risk of 3%. Affects ages 3-8, males to females 2:1 [3]. Typically well appearing with normal labs, however, this is a diagnosis of exclusion and a septic joint should be ruled out. Management includes NSAID use and return to activity as tolerated [4].
Septic Arthritis - A “do not miss” diagnosis, commonly ages 3-6 with a slight male predominance [5]. Typically presenting with fevers and abnormal labs. The Kocher Criteria (originally developed in 1999 and validated in 2004) can be helpful in determining the likelihood of septic arthritis [6]. Management includes imaging studies, typical ultrasound to assess for a joint effusion, then a diagnostic arthrocentesis & antibiotics. The antibiotic regimen should be tailored to the child’s age and other predisposing factors to certain pathogens.



Osteomyelitis - Occurs in 1:5000-7700 kids in increased prevalence with MRSA communities; 2:1 male to female predominance with half of all cases occurring in ages less than 5 [7]. Commonly hematogenous spread from bacteremia; clinical suspicion should prompt radiologic evaluation. X-rays may be likely to be normal/inconclusive early in the disease course and MRI may be often indicated. Labs can be helpful but are not specific; a systematic review of >12,000 patients showed that elevated WBC was only present in 36% of patients [7]. ESR and CRP are non-specific but have a sensitivity of 95% [7]. Antibiotic therapy guidelines are similar to the management of septic arthritis. Surgical intervention may be indicated if there is a lack of improvement after 48-72 hours [8].

Osteomyelitis of the distal tibia (orthobullets.com)
Orthopedic
Legg-Calve-Perthes / Avascular Necrosis of the Hip - Age range 3-12 with a peak at 5-7, male to female ratio 3:1, can be bilateral in 10-20% of patients [9]. Radiographs should be obtained with high clinical suspicion but are often normal early in the course. An MRI would show fragmentation of the femoral head. The patient should be made non-weight bearing and be referred to a specialist. Children under 8 typically have a better prognosis however long-term management is poorly defined as there has been no long-term study [10].

Avascular necrosis of bilateral hip (orthobullets.com)


SCFE of left hip (orthobullets.com)
Slipped Capital Femoral Epiphysis - Typically obese child, median age 12, bilateral in 20-40% of cases [11]. Presentation is classically chronic hip pain with antalgic gait however may present with knee pain. Physical exam classically shows external rotation and abduction of the hip during hip flexion. Management is orthopedic consultation for operative stabilization [12].
References
Smith E, Anderson M, Foster H. The child with a limp: a symptom and not a diagnosis. Archives of disease in childhood - Education & practice edition. 2012;97(5):185-193. doi:10.1136/archdischild-2011-301245.
Naranje S, Kelly DM, Sawyer JR. A Systematic Approach to the Evaluation of a Limping Child. Am Fam Physician. 2015 Nov 15;92(10):908-16. PMID: 26554284.
Landin LA, Danielsson LG, Wattsgård C. Transient synovitis of the hip. Its incidence, epidemiology and relation to Perthes' disease. J Bone Joint Surg Br. 1987;69(2):238-242.
Kermond S, Fink M, Graham K, Carlin JB, Barnett P. A randomized clinical trial: should the child with transient synovitis of the hip be treated with nonsteroidal anti-inflammatory drugs?. Ann Emerg Med. 2002;40(3):294-299. doi:10.1067/mem.2002.126171
Bennett OM, Namnyak SS. Acute septic arthritis of the hip joint in infancy and childhood. Clin Orthop Relat Res. 1992;(281):123-132.
Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm. J Bone Joint Surg Am. 1999;81(12):1662-1670. doi:10.2106/00004623-199912000-00002
Dartnell J, Ramachandran M, Katchburian M. Haematogenous acute and subacute paediatric osteomyelitis: a systematic review of the literature. J Bone Joint Surg Br. 2012;94(5):584-595. doi:10.1302/0301-620X.94B5.28523
Kaplan SL. Osteomyelitis in children. Infect Dis Clin North Am. 2005;19(4):787-vii. doi:10.1016/j.idc.2005.07.006
Johansson T, Lindblad M, Bladh M, Josefsson A, Sydsjö G. Incidence of Perthes' disease in children born between 1973 and 1993. Acta Orthop. 2017;88(1):96-100. doi:10.1080/17453674.2016.1227055
Canavese F, Dimeglio A. Perthes' disease: prognosis in children under six years of age. J Bone Joint Surg Br. 2008 Jul;90(7):940-5. doi: 10.1302/0301-620X.90B7.20691. PMID: 18591607.
Herngren B, Stenmarker M, Vavruch L, Hagglund G. Slipped capital femoral epiphysis: a population-based study. BMC Musculoskelet Disord. 2017;18(1):304. Published 2017 Jul 18. doi:10.1186/s12891-017-1665-3
Reynolds RA. Diagnosis and treatment of slipped capital femoral epiphysis. Curr Opin Pediatr. 1999;11(1):80-83. doi:10.1097/00008480-199902000-00016
Expert Commentary
Thank you to Drs. Ng and Bigach for compiling a concise approach to a common chief complaint encountered by Emergency Physicians across the county: a child with a new limp or the refusal to bear weight.
The first step to this often-challenging problem is to try to localize the pain, and in non-verbal kiddos, this can be the most difficult task. As highlighted above, if the child is able, observe their ambulation and establish laterality of the limp and when it occurs during the gait cycle. Most of the disease processes we as Emergency Physicians are concerned about will cause an antalgic gait or a shortened stance phase. Shortening the stance phase decreases the amount of time that the child is bearing weight on the painful limb in an effort to decrease their pain. Sometimes this is so effective that their parents will observe a limp, but the child will not complain of any pain. A thorough exam of the back and lower extremities including inspection, palpation, and range of motion of all joints is also imperative for trying to localize the cause of their symptoms.
Let your exam and history guide lab evaluation and imaging, however, a good place to start is usually basic labs and inflammatory markers and a plain film of the affected joint. In some cases, you won’t be able to localize pain or exam findings at all, and a broad workup including plain film imaging of the entire extremity may be necessary.
A few additional pearls:
Always consider non-accidental trauma in children with new limp or refusal to bear weight.
Systemic symptoms such as fever should raise your suspicion for infectious etiology such as osteomyelitis or septic arthritis.
Classically children with transient synovitis will have had a recent viral illness, but this is not always the case.
Always examine the hips and consider hip plain films in children complaining of knee or thigh pain, but with a benign knee exam. They could be hiding an SCFE or Leg-Calve-Perthes disease.
Don’t forget to examine the SI joint, as it too can become infected or inflamed.
History of night pain should raise your antenna for malignancy like osteosarcoma, Ewing’s sarcoma, or leukemia.
Consider Lyme arthritis in your differential for joint pain and swelling in endemic areas.
Ultrasound can be useful when evaluating for septic arthritis and transient synovitis and can be performed at the bedside. However, both septic arthritis and transient synovitis can cause effusion, and therefore it is not useful in differentiating between the two. (That’s where the Kocher Criteria should be used to risk-stratify and determine if joint aspiration and fluid analysis are warranted)

Ultrasound evaluation of a pediatric hip joint demonstrating effusion courtesy of Dr. Maulik S Patel (https://radiopaedia.org)
Finally, make sure that the parents understand the diagnosis, expected course, and follow-up plan. If the child continues to refuse to bear weight, their symptoms worsen or do not improve, or they develop new concerning symptoms such as new fever or new urinary retention, they should return to the Emergency Department or their pediatrician for re-evaluation. More than once I’ve had patients who seemed for all the world to have transient synovitis eventually be diagnosed with spinal cord tumor, chronic recurrent multifocal osteomyelitis, etc.

Terese Whipple, MD
Assistant Professor
Department of Emergency Medicine
University of Iowa Hospitals and Clinics
How To Cite This Post:
[Peer-Reviewed, Web Publication] Ng, T. Bigach, P. (2021, Dec 20). Hip Pain in Pediatrics. [NUEM Blog. Expert Commentary by Whipple, T]. Retrieved from http://www.nuemblog.com/blog/hippainpediatrics
Other Posts You May Enjoy
Featured



Kawasaki Disease

Written by: Richmond Castillo, MD (NUEM ‘23) Edited by: Andra Farcas (NUEM ‘21) Expert Commentary by: Wee-Jhong Chua, MD

Expert Commentary
A great summary of a rare, but important illness to consider in children with prolonged fevers. Kawasaki disease is a vasculitis to small and medium vessels, often occurring in childhood. While most children recover, there are important cardiac complications that need to be considered. Treatment with IVIG within the first 10 days of illness has been shown to reduce the prevalence of coronary artery aneurysms. In fact, untreated disease has been associated with an incidence of coronary artery aneurysm as high as 25%. [1]
The diagnosis of this disease process is challenging as there are no definitive testing methodologies and even the etiology of the systemic inflammatory process remains unknown. While most guidelines include 5 days of fever, the 2017 American Heart Association Scientific Statement indicates that 4 days of fever with the corresponding clinical features can be diagnostic. Moreover, in rare instances experienced clinicians have been able to make the diagnosis as early as 3 days. [1] In clinical practice, the clinical pathways at leading children’s hospitals use 4 days as a threshold for evaluation with the presence of 4 or 5 principal clinical features are present. [2,3] However, the standard practice continues to be 5 days for the classic diagnosis.
With high clinical suspicion for Kawasaki Disease, transfer to a pediatric hospital should be considered with consultations with Infectious Disease, Cardiology, and Rheumatology. It is important to have a high clinical suspicion for Kawasaki disease in children with prolonged fevers.
References
McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17):e927-e999. doi:10.1161/CIR.0000000000000484
D. Whitney, MD; K. Dorland, BSN; J. Beus, MD; J. Brothers, MD; L. Buckley, MD; S. Burnham MD; D. Campeggio, MSN; K. DiPasquale, MD; H. Ghanem MD; J. Hart MD; J. Lavelle, MD; C. Law PharmD; S. Natarajan, MD; J. Ronan, MD; V. Scheid, MD; S. Swami, MD; H. Ba C. Kawasaki Disease or Incomplete Kawasaki Disease Clinical Pathway — Emergency Department and Inpatient | Children’s Hospital of Philadelphia. Accessed October 20, 2020. https://www.chop.edu/clinical-pathway/kawasaki-disease-incomplete-kawasaki-disease-clinical-pathway
Seattle Children’s Hospital, M Portman, M Basiaga, E Beardsley, R Engberg, K Hayward, K Kazmier, M Leu, R Migita, J Rasiah, R Sadeghian, S Sundermann, S Vora, S Zaman, 2018 February. Kawasaki Disease Pathway. Available from: http://www.seattlechildrens.org/pdf/Kawasaki-Disease-Pathway.pdf

Wee-Jhong Chua, MD
Attending Physician, Pediatric Emergency Medicine
Ann & Robert H. Lurie Children's Hospital of Chicago
How To Cite This Post:
[Peer-Reviewed, Web Publication] Castillo, R. Farcas, A. (2021, Feb 1). Kawasaki Disease. [NUEM Blog. Expert Commentary by Chua, W]. Retrieved from http://www.nuemblog.com/blog/kawasaki-disease.
Other Posts You May Enjoy






Preterm Neonatal Resuscitation
Written by: Aaron Wibberley, MD (NUEM ‘22) Edited by: Vidya Eswaran, MD '20 Expert Commentary by: Spenser Lang, MD

Expert Commentary
Thanks to Dr. Wibberley and Dr. Eswaran for providing this infographic on a tough topic – neonatal resuscitations.
Usually, deliveries in the emergency department cause a dichotomy of emotions – initial anxiety, then relief and happiness. Most of our deliveries tend to be quick, precipitous, with hopefully just enough warning for us to grab gloves and remember where the baby warmer is. Unfortunately, when babies decide to struggle with their first few minutes of life, this becomes a lot more stressful for everyone.
Fair warning – though I am an emergency medicine physician, and prepared to deal with emergent situations of any age, I think there are very few of us who feel as comfortable with neonatal resuscitations as we do with critically ill trauma or cardiac arrest patients. Especially if your department sees very little pediatrics, it is completely normal to feel anxiety when imagining resuscitating a neonate, and even more so a pre-term baby. This is OK! In fact, this should motivate you to get familiar with NRP, and provides a perfect opportunity for spaced repetition throughout your career to enhance recall.
Here are my broad strokes steps for a fresh neonate requiring resuscitation.
#1: Know your resources! The first step in managing a neonatal resuscitation occurs far before the patient shows up in your department. Where is your baby warmer? Where are your teeny-tiny BVM’s? What’s the smallest ETT and intubating blade you stock, and where? I promise you, the hardest part of intubating this baby won’t be the actual mechanics of placing an ETT – it will be in the preparation and supply gathering. Don’t rely on your nurses to know everything when seconds count – know where this stuff is yourself.
#2: Call for help, early and often. Many emergency departments have some type of OB/imminent delivery response – hopefully this brings in a pediatrician well trained in neonatal resuscitation as well. Hopefully, this also brings a nurse who is used to placing IV’s in these itty bitty babies. If this doesn’t describe your hospital, call to start the transfer process, and move on to #3…
#3: Dry and stim. Nearly all babies respond to drying and stimulation. Please don’t start bagging a poor newborn before drying it off and giving it a good rub for 30-60 seconds (unless it’s extremely pre-term – try to avoid rubbing all the skin off of a 25-weeker, this is bad form.) At the same time, keep in mind that these babies will need some form of external thermoregulation so make sure the warmer is actually functioning.
#4: When in doubt, fix the breathing. As is obvious when scanning through NRP guidelines, 95% of managing a sick newborn lies in assisting the respirations. Poor tone? Fix the breathing. Initial HR below 100? Try to fix the breathing. Poor color? You get it. Don’t be afraid to escalate from blow by, to PEEP, to BVM. If the baby has little to no respiratory effort, a couple initial breaths via BVM can quickly improve the situation. But please, when you’re bagging a tiny neonate, use small breaths – this is not the typical 120 kg patient we are used to.
#5: In the short term, an IO is your friend. A UVC is golden, but not really possible in an active resuscitation. The good news is that most babies don’t need IV access in the short term – for my reasoning, see #3 and #4. The literature suggests that placing the neonatal IO in the proximal tibia, distal tibia, or distal femur can be safe and effective.
#6: This is the time to debrief. Whether a happy or a tragic ending, this is a rare and emotional event in the emergency department. Debrief with your team. Talk to whoever you talk to about this stuff – spouse, friend, coworker. We are champions of compartmentalization in the emergency department out of necessity, but don’t bear the entirety of these encounters on yourself – lean on those around you.

Spenser Lang, MD
Assistant Professor
Department of Emergency Medicine
University of Cincinnati
How To Cite This Post:
[Peer-Reviewed, Web Publication] Wibberly, A. Eswaran, V. (2020, Nov 9). Preterm Neonatal Resuscitation. [NUEM Blog. Expert Commentary by Lang, S]. Retrieved from http://www.nuemblog.com/preterm-neonatal-resuscitation
Other Posts You May Enjoy
Little Lungs, Little Differences: Initiating Emergency Department Mechanical Ventilation in the Pediatric Patient
Written by: Matt McCauley MD (PGY-3) Edited by: Jacob Stelter, MD (NUEM ‘19) Expert commentary by: Katie Wolfe, MD
Airway management of pediatric patients is a reasonable source of anxiety for the emergency physician. Children are intubated three to six times less often than adult emergency department patients [1]. Hence, it stands to reason that EP experience with mechanically ventilated children can be scarce [2] . Additionally, evidence driven practice in pediatric mechanical ventilation is limited and practice patterns vary between institutions and providers. These unknowns can make the prospect of managing these patients even more intimidating [3]. However, pediatric ventilator management is largely driven by data extrapolated from adults, which should come as a relief to the EP [4]. By keeping in mind small differences in pediatric physiology and keeping the consulting intensivist (and Broselow Tape) close at hand, an EP can effectively initiate mechanical ventilation in the smallest and most anxiety-provoking patients.
Getting Help
Like the Fat Man said in House of God: “[Disposition] comes first.” The intubated child is bound for a pediatric ICU and hopefully the accepting pediatric intensivist is already aware of any intubated patient and can be a great deal of help and support as you work together to make your patient safe for transfer upstairs or across town. Although the use of a Broselow tape and other height based methods of estimating body weight for drug dosing is fraught with error 5, the Broselow’s color coding allows for quick estimation of ideal body weight (IBW) that is required to calculate ideal tidal volumes.
Choosing a Mode
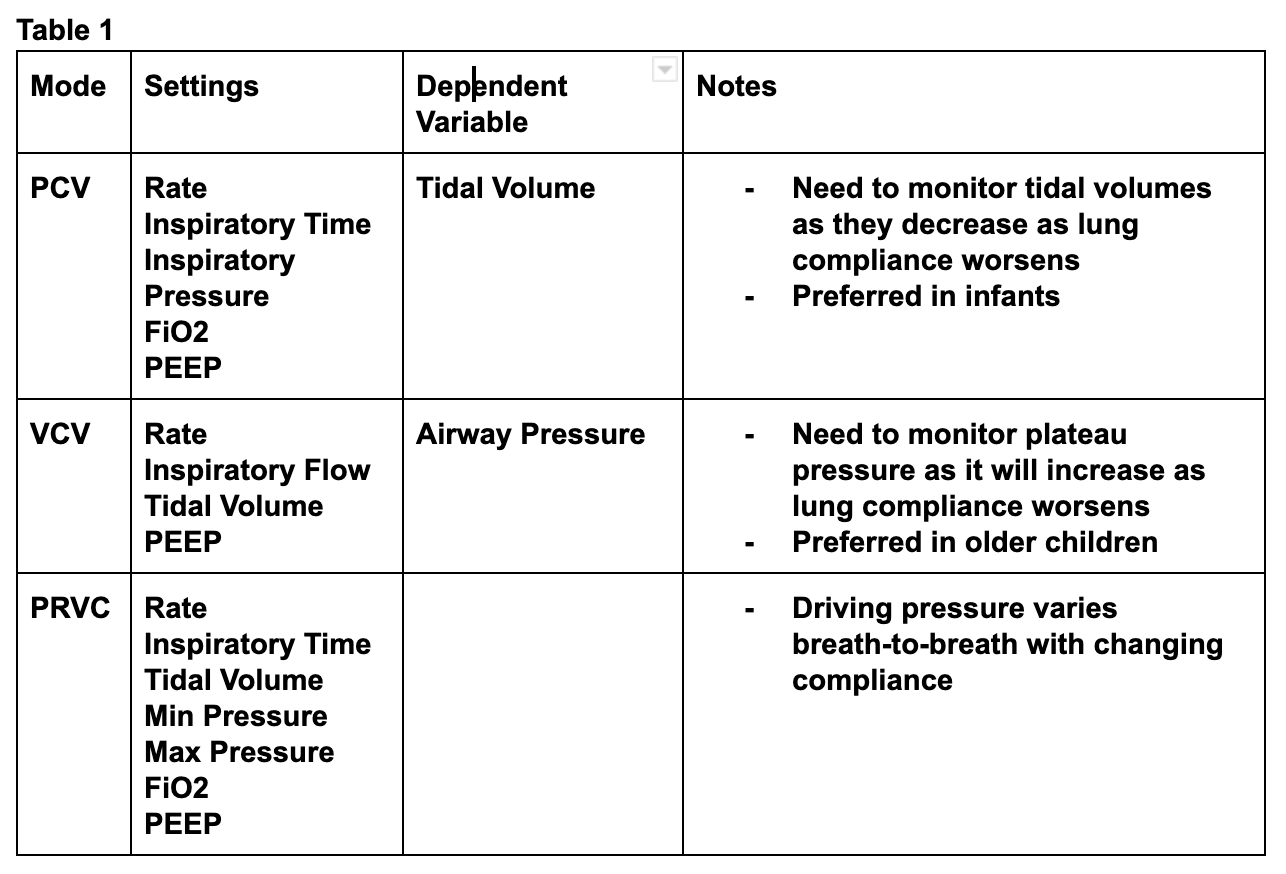
As mentioned, practice patterns related to pediatric ventilator management vary greatly [3]. The most commonly used modes for emergency pediatric ventilation include pressure assist control ventilation (PCV), volume control ventilation (VCV), and pressure regulated volume control ventilation (PRVC) [2]. PCV is typically favored in neonates and infants while volume modes are preferred in larger children [2]. When utilizing PCV, the provider sets the, inspiratory rate, inspiratory time, and inspiratory pressure meaning that the delivered tidal volume is dependent on the lung compliance of the patient [6]. This means that worsening compliance results in low tidal volumes. (Table 1)
Vt = Compliance x Delta Pressure
In contrast, VCV ventilation requires that the physician set the inspiratory rate, inspiratory flow rate, tidal volume, and PEEP. The ventilator delivers a fixed flow of air until the desired tidal volume is reached. This means that worsening compliance results in higher airway pressures (Table 1) [1]. The final commonly used mode for ventilating pediatric lungs is PRVC which, rather than requiring a set inspiratory flow rate like most volume controlled modes, utilizes a set inspiratory time, a targeted tidal volume, and a range of allowed pressures. With each breath the ventilator delivers a decelerating breath over the set time at an inspiratory pressure within the allowed range. If the resulting tidal volume is too high, the next breath is delivered with less pressure, if the volume falls short of the targeted tidal volume, the next breath is delivered with more pressure (Table 1) [6].
Finally, synchronized intermittent mandatory ventilation (SIMV) is often added to the above modes in pediatric ventilation. In SIMV, any time the patient initiates breaths within the set respiratory rate, a pressure supported breath (usually at 5-10 mmHg) is given rather than the full volume or pressure controlled breath. Pediatric patients are more likely than their adult counterparts to over-breathe the set respiratory rate, putting them at risk of breath stacking from large volume breaths. SIMV can help to mitigate this risk [2]. Despite all this complexity, there is a paucity of good evidence for or against any particular mode for ventilation the critically ill child [4]. This should reassure the EP to choose their most familiar ventilator mode in conjunction with their intensivist.
Choosing Age-Appropriate settings
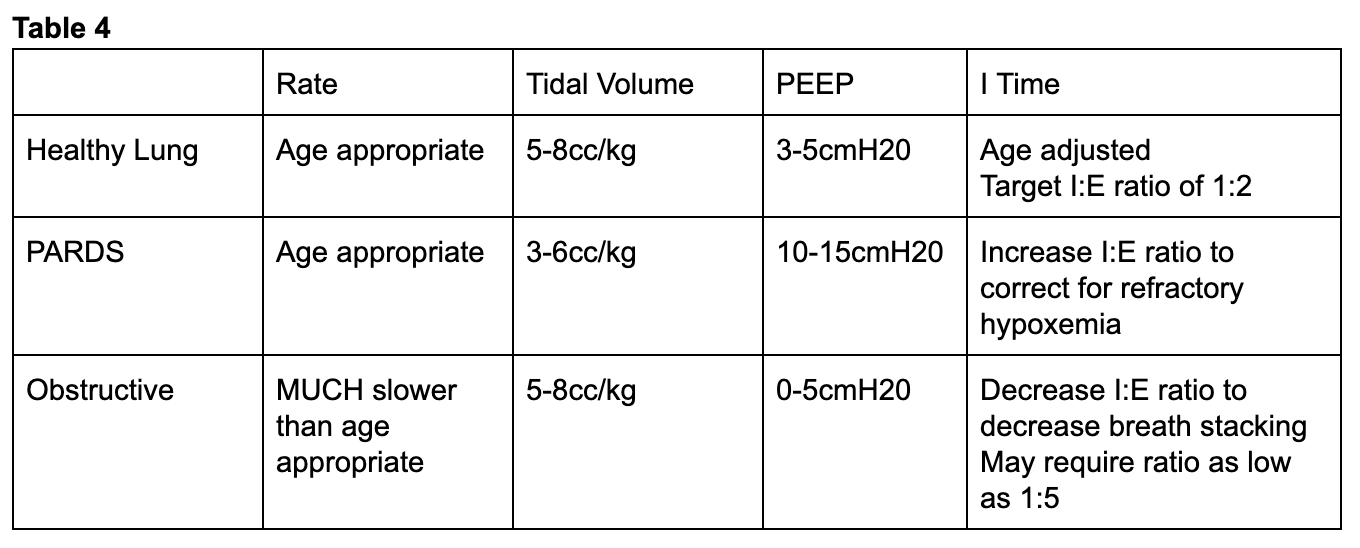
Since pediatric respiratory rates vary wildly from adults, one should take the patient’s age into account when initiating mechanical ventilation (table 2) . With the exception of children with obstructive pathophysiology, the physician should attempt to match the patient’s pre-intubation minute ventilation [2]. Tidal volume goals for pediatric patients do not vary much from adults with most data being extrapolated from adult studies [4] and large trials have been unable to establish as safe threshold for tidal volume [8]. The Pediatric Acute Lung Injury Consensus Conference (PALICC) recommends targeting 5-8cc/kg of ideal body weight (IBW) for most children either by setting a tidal volume in VCV or altering driving pressures for pressure controlled modes to target tidal volumes in this range for most patients [9]. Just as in adult patients, the intubating physician can set initial FiO2 at 100% to overcome hypoxia caused by peri-intubation apnea and then quickly down titrate targeting a SpO2 of 92-97% [9] .

If ventilating pediatric patients with pressure controlled ventilation, initially inspiratory times can be found on the Broselow or in a PALS manual 10 (table 3). If a volume controlled mode of ventilation is desired, inspiratory flow can be titrated to achieve a inspiratory to expiratory time ratio of 1:2 [2]. After initial setup, arterial blood gas analysis, continuous end-tidal CO2 measurement, and a chest X ray to evaluate tube positioning are just as critical here as they are in the adult patient.

Ventilating the Child with Refractory Hypoxemia
While most pediatric patients will be relatively straightforward to ventilate, the patient intubated for infectious pathologies like pneumonia or bronchiolitis is at risk for ARDS and should be approached with lung-protective ventilation strategies in mind. Victims of drowning are similarly at risk and fall under the category of patients requiring lung-protective settings [11]. There is no pediatric equivalent for the ARDSnet trial [12] so adult data has been extrapolated to be applied to pediatric patients [3] making this familiar territory for the adult emergency physician.
While most children will tolerate levels of PEEP between 3-5cmH204, PALICC recommends that children at risk of ARDS receive moderately elevated levels of PEEP between 10-15cmH2O with an SPO2 goal between 88-92% for kids requiring PEEP more than 10mmH2O [9]. In order to assess the extent of lung injury, an inspiratory hold maneuver can be used to determine lung compliance which is typically 1.5-3.0/cmH2O/kg for an infant [2]. If the EP notes decreased compliance, tidal volumes closer to 3-6cc/kg should be targeted [9]. If these measures fail to improve oxygenation, inspiratory time can be increased in order to target an inspiratory to expiratory ratio closer to 1:2. With the exception of children with elevated intracranial pressure (ICP), congenital heart disease, or pulmonary hypertension, permissive hypercapnea is acceptable as long as the pH remains > 7.2 [4].
Ventilating the Child with Obstructive Physiology
Endotracheal intubation of the asthmatic child is thankfully a rare event but one that portends to a high mortality [13]. At baseline, children exhibit higher airway resistance than their adult counterparts [2] and the even higher airway resistance in asthmatic patients creates high levels of intrinsic PEEP while increases the risk of breath stacking and pneumothorax [14]. If the patient’s respiratory rate is too high, lungs will remain progressively inflated at end expiration. This increases intra-thoracic pressure thereby decreasing preload and precipitating cardiovascular collapse. The level of this intrinsic PEEP can be assessed with an expiratory hold maneuver (Figure 1). To do this, the ventilator occludes the expiratory port at the end of exhalation allowing the alveolar and airway pressures to equilibrate. The total pressure at this moment minus the set PEEP on the ventilator represents the intrinsic PEEP [7]. More simply, a flow/time curve that fails to return to baseline prior to the onset of inspiration may signal to the EP that there may be high levels of intrinsic PEEP 2. (Figure 2)


To counteract this, asthmatics and other patients with obstructive physiology will need respiratory rates far below median age values. In one series of asthmatic children aged as young as nine months, rates as low as 8-12 breaths per minute were used [15]. In order to further facilitate full expiration, the I:E ratio should be increased to target values as low as 1:4-5 [15]. High levels of PEEP are typically not required in these patients and use of low to zero PEEP has been documented [14]. Hypercapnea should be expected and is allowable in these patients [14].
Prolonged mechanical ventilation of the pediatric patient exhibits far more complexities than this blog post covers and is beyond the scope of most emergency medicine practice. However, by relying on evidence driven practice for adult intubated patients with close guidance from a pediatric intensivist and pediatric resuscitation reference, the initial steps and safe monitoring of the intubated child are well within the abilities of the emergency physician.
Expert Commentary
Thank you for this concise summary of mechanical ventilation in children. As noted, while this is an infrequent occurrence, the initial management of a ventilated child is incredibly important.
In choosing initial ventilator settings, the key is decision and reassessment. Most modes of ventilation will work in most children. However, careful attention to what support you’re providing your patient with and what the results of that support are, is vital. Personally, I like using PRVC mode because it adjusts support in children with changing lung compliance without a lot of manipulation required by the physician. But, in any mode of ventilation you can make adjustments as you note changes in compliance. In pressure mode, watch your tidal volumes and in volume control or PRVC, monitor your peak pressures (along with your saturations and end tidal) to see if you’re achieving your goals. Use of SIMV versus AC modes of ventilation are important in the weaning phase of ventilation but less important as you’re initiating mechanical ventilation as the patient is typically neuromuscularly blocked. I also want to emphasize the importance of weaning supplemental oxygen as soon as possible in order to understand the adequacy of your support from an oxygenation and ventilation standpoint. Hypoxemia is bad but so is hyperoxia and masking hypoventilation.
While the research in pediatric ARDS is not as robust as in adults, there is a growing body of literature describing epidemiology and current practice.[1] Current management strategies continue to be extrapolated from adult data- including lung protective strategies of permissive hypoxemia and hypercarbia (tidal volumes 3-6 cc/kg, saturations >92% in mild pARDS and >88% in severe pARDS, pH > 7.2 with exceptions for specific populations including those with pulmonary hypertension).[2] Restrictive fluid strategies (after initial resuscitation) and adequate sedation are recommended. There is ongoing research regarding the use of HFOV and prone positioning in pARDS but this is outside the scope of emergency department care.
The intubated asthmatic remains a source of anxiety among many pediatric intensivists. Key takeaways are low respiratory rate to allow for full exhalation and prevent air trapping and matching intrinsic PEEP. Permissive hypercapnia is appropriate in these patients and their CO2 should be measured by blood gas; recognizing that there is a significant amount of dead space and end tidal may be falsely reassuring/low. When intubating patient with obstructive physiology, it’s also important to ensure adequate preload and have a high suspicion for pneumothorax if they decompensate. Utilizing ketamine for sedation can be useful in these patients and has the advantages of bronchodilation and not significantly suppressing their respiratory drive, allowing them to participate in setting their inspiratory/expiratory times.
Final thought: don’t hesitate to ask for help- from the pediatric intensivists in house or over the phone- we are happy to collaborate!
References:
Khemani RG, Smith L, Lopez-Fernandez YM, et al. Paediatric acute respiratory distress syndrome incidence and epidemiology (PARDIE): an international, observational study. Lancet Respir Med. 2019 Feb;7(2):115-128. doi: 10.1016/S2213-2600(18)30344-8. Epub 2018 Oct 22.
Orloff KE, Turner DA, Rehder KJ. The Current State of Pediatric Acute Respiratory Distress Syndrome. Pediatr Allergy Immunol Pulmonol. 2019 Jun 1; 32(2): 35–44. doi: 10.1089/ped.2019.0999. Epub 2019 Jun 17.

Dr. Katie Wolfe, MD
Attending Physician
Pediatric Critical Care
Ann & Robert H. Lurie Children's Hospital of Chicago
Instructor of Pediatrics (Critical Care)
Northwestern University Feinberg School of Medicine
How To Cite This Post
[Peer-Reviewed, Web Publication] McCauley, M. Stelter, J. (2020, Feb 3). Initiating Emergency Department Mechanical Ventilation in the Pediatric Patient. [NUEM Blog. Expert Commentary by Wolfe, K]. Retrieved from http://www.nuemblog.com/blog/ped-mech-vent.
Other Posts You Might Enjoy…
References
Losek J.D., Olson L.R., Dobson J.V., et al: Tracheal intubation practice and maintaining skill competency: survey of pediatric emergency department directors. Pediatr Emerg Care 2008; 24: pp. 294-299
Pacheco, G. S., Mendelson, J., & Gaspers, M. (2018). Pediatric Ventilator Management in the Emergency Department. Emergency Medicine Clinics of North America, 36(2), 401–413. https://doi.org/10.1016/j.emc.2017.12.008
Rimensberger, Peter C., Ira M. Cheifetz, and Martin C. J. Kneyber. “The Top Ten Unknowns in Paediatric Mechanical Ventilation.” Intensive Care Medicine 44, no. 3 (2018): 366–70. https://doi.org/10.1007/s00134-017-4847-4
Kneyber, Martin C. J., Daniele de Luca, Edoardo Calderini, Pierre-Henri Jarreau, Etienne Javouhey, Jesus Lopez-Herce, Jürg Hammer, et al. “Recommendations for Mechanical Ventilation of Critically Ill Children from the Paediatric Mechanical Ventilation Consensus Conference (PEMVECC).” Intensive Care Medicine 43, no. 12 (December 2017): 1764–80. https://doi.org/10.1007/s00134-017-4920-z.
Wells et al. The accuracy of the Broselow tape as a weight estimation tool and a drug-dosing guide – A systematic review and meta-analysis. Resuscitation. 2017 Dec;121:9-33.
Singer, BD. Corbridge, TC. "Pressure modes of invasive mechanical ventilation" Southern Medical Journal" 104, no. 10 October 2011, pp 701-709
Singer, BD. Corbridge, TC. "Basic Mecahnical Ventilation" Southern Medical Journal" 102, no. 12 December 2009 , pp pp 1238-1245
de Jager P, Burgerhof JG, van Heerde M, et al: Tidal volume and mortality in mechanically ventilated children: A systematic review and meta-analysis of observational studies*. Crit Care Med 2014; 42:2461–2472
Rimensberger PC, Cheifetz IM. Ventilatory support in children with pediatric acute respiratory distress syndrome: proceedings from the pediatric acute lung injury consensus conference. Pediatr Crit Care Med.(2015) 16(5 Suppl. 1):S51–60. 10.1097
Chameides L, Samson RA, Schexnayder SM, Hazinski MF (Eds).Pediatric Advanced Life Support Provider Manual, , American Heart Association, Dallas 2012.
Semple-Hess, J., & Campwala, R. (2014). Pediatric submersion injuries: emergency care and resuscitation. Pediatric Emergency Medicine Practice, 11(6), 1–21
Kneyber, Martin C. J. “Mechanical Ventilation for Pediatric Acute Respiratory Distress Syndrome: Few Known Knowns, Many Unknown Unknowns.” Pediatric Critical Care Medicine: A Journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies 17, no. 10 (2016): 1000–1001.
Rampa S, Allareddy V, Asad R, et al. Outcomes of invasive mechanical ventilation in children and adolescents hospitalized due to status asthmaticus in United States: a population based study. J Asthma 2015; 52:423.
Rubin, Bruce K., and Vladimir Pohanka. “Beyond the Guidelines: Fatal and near-Fatal Asthma.” Paediatric Respiratory Reviews 13, no. 2 (June 2012): 106–11. https://doi.org/10.1016/j.prrv.2011.05.003.
Cox, R. G., G. A. Barker, and D. J. Bohn. “Efficacy, Results, and Complications of Mechanical Ventilation in Children with Status Asthmaticus.” Pediatric Pulmonology 11, no. 2 (1991): 120–26
Pediatric Ankle Injuries
Written by: Nikita Patel, MD (NUEM PGY-2) Edited by: Paul Trinquero, MD (NUEM ‘19) Expert commentary by: Kristen Loftus, MD, MEd
Expert Commentary
This is a succinct, high-yield review of pediatric ankle injury management. I appreciate the focus on radiograph-negative injuries, as only a minority will have a fracture identified on radiographs (~12%).
You highlight a key point about the use of the Ottawa Ankle Rules (OAR). A few things I would emphasize/add:
You most definitely do not need an x-ray on every pediatric patient with an ankle injury (though x-rays are obtained ~85-95% of the time).
The OAR have indeed been well-validated in children. In clinical practice, the problem you run into with the pediatric population is that: 1) kids commonly refuse to bear weight even with mild ankle injuries and 2) in pediatric patients (as opposed to adults), isolated distal fibular tenderness typically suggests a low risk ankle injury where x-rays won’t change your management.
The Low Risk Ankle Rule (LRAR) addresses these 2 key issues of using the OAR in kids, and it may be worth considering adopting the use of this clinical decision rule for pediatric ankle injuries. It was initially validated in children and is associated with a larger decrease in unnecessary radiographs compared to the OAR. [Boutis K, Komar L, Jaramillo D, et al. Sensitivity of a clinical examination to predict need for radiography in children with ankle injuries: a prospective study. Lancet. 2001;358:2118-21.]
No discussion on pediatric orthopedic injuries would be complete without a review of the Salter-Harris classification. There is a lot of practice pattern variation in the management of patients with negative radiographs but growth plate tenderness on exam (i.e. the potential Salter-Harris I fracture). The Boutis et al. group has done some great work in this area, and you highlight several key studies in your excellent review of the literature. I personally feel well-supported by this emerging evidence, and my practice pattern is to place patients in a removable ankle lacer (if able to bear weight) or a pneumatic walking boot (if unable to bear weight), with crutches as needed, and outpatient follow-up with their pediatrician versus Sports Medicine, rather than Orthopedics.

Kirsten V. Loftus, MD MEd
Division of Pediatric Emergency Medicine
Ann and Robert H. Lurie Children’s Hospital of Chicago
How to Cite This Post
[Peer-Reviewed, Web Publication] Patel N, Trinquero P. (2019, Oct 21). Pediatric Ankle Injuries. [NUEM Blog. Expert Commentary by Loftus K]. Retrieved from http://www.nuemblog.com/blog/peds-ankle.
Other Posts You May Enjoy
Non-Accidental Trauma - A Can’t Miss Diagnosis
Written by: Dana Loke, MD (NUEM PGY-4) Edited by: Ashley Amick, MD (NUEM ‘18) Expert commentary by: Lauren Riney, DO
Introduction
Non-accidental trauma (NAT) is a leading cause of pediatric traumatic injury and death. In 2014 alone, there were 1546 reported deaths from NAT and 3.6 million child abuse referrals submitted to Child Protective Services (CPS). [1] NAT is most commonly encountered in young children, but can occur at any age. The classic signs and symptoms of NAT will be reviewed here, but it is important to realize that occult injury is common. Compared with accidental pediatric trauma, patients with NAT have been shown to have higher injury severity scores, rates of intensive care unit admission, and mortality. Furthermore, the diagnosis of NAT is delayed in 20% of cases, increasing the risk of poor outcomes.[2] Therefore, the Emergency Physician (EP) must maintain a high index of suspicion for NAT to prevent the grave consequences of missed diagnosis for the patient and any other children in the home.
Red Flags and Risk Factors
NAT is a frequently missed diagnosis, but there are some red flags and risk factors that should make the EP take pause and consider this diagnosis. Children at greatest risk are generally toddler and younger, and often come from dysfunctional family units. A recent study found that 97% of NAT cases have antecedent familial dysfunction, such as substance abuse (alcohol or drugs), psychiatric disorder, history of violence or incarceration, or child withdrawal. [3] Additionally, over 70% of reported NAT deaths in 2014 were in children under 3 years old. [1]
Red Flags
Injuries inconsistent with the caregiver’s history
Reported mechanism of injury is unexpected for the child’s developmental status (for instance, a 2 week old infant rolling off of a bed)
Delayed presentation
Risk Factors
Age under 5 account for 81.5% of cases; children under 1 are most vulnerable [3]
Prematurity
Multiple medical conditions
Young parent
Female parent (although males are more likely to inflict fatal NAT)
Poor social support
Unplanned or unwanted pregnancy
Poor prenatal care
Shorter birth intervals between children
Increased number of separations from the child in the first year
Abuser Characteristics
Poor self-esteem
Depression and suicide attempts
Life stressors
Personal history of being abused as a child
Exposure to foster care or abandonment as a child
Engagement in criminal activity or corporal punishment as a child
Many other suspected risk factors have been studied. There is no consensus regarding whether a particular race is at greatest risk for NAT however black children have a greater risk of mortality from NAT. [4] Similarly, there is no consensus regarding socioeconomic status as it relates to NAT risk, but studies have shown that incidence of non-accidental head trauma and its severity rise during times of economic recession. [4]
Presentation
![Figure 1: Bruising patterns that suggest child abuse. [6]](https://images.squarespace-cdn.com/content/v1/549b0d5fe4b031a76584e558/1570459114532-IVTA7KT3PX1J6DGC3U3L/Figure+1%3A+Patterns+of+Bruising)
Figure 1: Bruising patterns that suggest child abuse. [6]
Bruising
Bruising is the most common manifestation of NAT but has low specificity. In any child presenting with bruising, it is imperative to note the location, shape and pattern of the lesion and ensure this is clearly documented. Bruising located over soft tissue areas such as the cheeks, neck, genitals, buttocks, torso, and back, are more likely to represent NAT than bruises over bony prominences. [4] The shape of the bruise should be considered as well, since the bruise often reflects the shape of the causative object. Common objects used to inflict injury include belts, cords, shoes, kitchen utensils, hangers, and teeth. [4] Additionally, patterned bruises should raise suspicion for NAT since they generally do not occur with accidental trauma. Lastly, any bruising in non-mobile infants is suspicious for NAT as well. [5]
![Figure 2: Forced immersion burn of buttocks with bilateral, symmetric leg involvement in a “stocking” pattern. [7]](https://images.squarespace-cdn.com/content/v1/549b0d5fe4b031a76584e558/1570459322548-EFHGSFQ962QP9FU5DNJN/Figure+2%3A+Burn+patterns+that+suggest+non-accidental+trauma)
Figure 2: Forced immersion burn of buttocks with bilateral, symmetric leg involvement in a “stocking” pattern. [7]
Burns
Burns occur in 8-12% of NAT cases. [2] The most common types of burns from NAT are scald burns and thermal contact burns. Scald burns are the most common and typically occur from forced immersion in hot liquids, usually of the buttock, or in a stocking-and-glove distribution. Scald burns generally have sharp demarcation, uniform depth, and lack splash or drip marks that would be seen in an accidental immersion. Thermal burns occur from contact with hot objects, of which branding with metal implements or cigarettes is a common presentation. Concerning features of burns include:
Location on the hands (especially the dorsum), legs, feet, or buttocks
Patterned contact burns in the shape of an object (such as a fork, clothing iron, curling iron, or cigarette lighter)
Sharp stocking-and-glove pattern with sparing of the flexed protected areas (the classic forced immersion burn pattern)
![Figure 3: Classic metaphyseal lesion. White arrows denote femoral metaphyseal separation and black arrow denotes a proximal tibial lesion or “bucket handle.” [1]](https://images.squarespace-cdn.com/content/v1/549b0d5fe4b031a76584e558/1570459580501-8461RMF0P9706GJW7XJU/Figure+3%3A+Fractures+of+NAT)
Figure 3: Classic metaphyseal lesion. White arrows denote femoral metaphyseal separation and black arrow denotes a proximal tibial lesion or “bucket handle.” [1]
Fractures
There are various non-accidental fracture patterns, several with high specificity as described below:
Classic metaphyseal lesion (CML) – Also known as “bucket handle fractures” or “corner fractures,” these fractures are highly specific in children less than one year old. They result from a shearing force applied to a long bone, which causes avulsion of the metaphysis. These fractures are not associated with falls.
Multiple posterior and/or lateral rib fractures – These fractures also have a high correlation with NAT in children less than one year old. They arise from a specific mechanism – grasping the child around the torso and exerting a squeezing/compressive force. These fractures are more likely to affect the rib head and neck given the closer proximity to the transverse processes of the spine. NAT should especially be considered when healing fractures are found in a child without recent CPR.
![Figure 4: Posterior and lateral rib fractures of differing ages indicative of NAT [4]](https://images.squarespace-cdn.com/content/v1/549b0d5fe4b031a76584e558/1570460464292-4QFTGMDQAB64NQBSYD9N/Figure+4%3A++Rib+fractures+of+differing+ages+indicative+of+NAT)
Figure 4: Posterior and lateral rib fractures of differing ages indicative of NAT [4]
Clavicular fractures and spiral fractures of long bones in nonambulatory children
Multiple fractures, especially if in different stages of healing
Scapular fractures
Sternal fractures
Spinous process fractures
Of note, spiral fractures of long bones generally result from twisting injuries (indicating NAT), but can occur accidentally from falls in ambulatory children. Therefore, these fractures (especially if coupled with clavicular fractures) are more specific for NAT in younger patients, and the specificity decreases with advancing age. Other described non-accidental patterns to consider include epiphyseal separations, vertebral body fractures and separations, digital fractures, linear and complex skull fractures, and subperiosteal bone formation. These patterns have low to moderate specificity for NAT. [1]
Abusive Head Trauma
Abusive head trauma (AHT) is the most fatal form of non-accidental injury in children. In fact, about 80% of deaths from NAT are caused by AHT and only 15% of patients with AHT survive without any sequelae. [4] AHT is a spectrum of injuries including collisions with stationary objects, direct blows to the head, and a repetitive acceleration- deceleration injury, also known as “Shaken Baby Syndrome.” Infants are particularly vulnerable to traumatic brain injury from shaking due to the relative weight of the head compared to the body, coupled with weak neck musculature. [1] If AHT is suspected, a non-contrast head CT should be obtained even with a nonfocal neurologic examination, because occult intracranial injury is common. Make sure to use age-appropriate dose reduction to minimize radiation exposure and if the CT scan is normal, consider further work-up with an MRI.
![Figure 5: Fundus of child with AHT with too-numerous-to-count retinal hemorrhages indicated by the black arrows. [8] The white arrow indicates small pre-retinal hemorrhages. The white arrowhead denotes hemorrhage extending into the peripheral retina…](https://images.squarespace-cdn.com/content/v1/549b0d5fe4b031a76584e558/1570460641270-3V7M52RMMV1QDMZ3PA1S/Figure+5%3A+Occular+manifestations)
Figure 5: Fundus of child with AHT with too-numerous-to-count retinal hemorrhages indicated by the black arrows. [8] The white arrow indicates small pre-retinal hemorrhages. The white arrowhead denotes hemorrhage extending into the peripheral retina. The black arrowhead denotes a healthy optic disc.
Ocular Manifestations
Although there are many ocular manifestations associated with non-accidental head injuries, retinal hemorrhages occur most often (about 60-85% of non-accidental head injuries). [4] Suspicion for NAT should be especially heightened when retinal hemorrhages are found in combination with signs of head trauma. Other ocular manifestations of NAT include periorbital hematoma, eyelid laceration, subconjunctival hemorrhage, subluxed or dislocated lens, cataracts, glaucoma, anterior chamber angle regression, iridiodialysis, retinal dialysis or detachment, intraocular hemorrhage, optic atrophy, or papilledema. [4]
Management and Disposition
All patients with suspected NAT should be admitted for protection and coordination of care even if they are clinically stable. Child Protective Services (CPS) must be notified, and engagement with the institutional social worker and child abuse team is recommended. It is important to note patients with NAT often have worse outcomes than other assault patients despite similar mechanisms of injury with intent to harm. [9] These patients often require close monitoring with Intensive Care Unit (ICU) resources. Patients with NAT should undergo a full skeletal survey as indicated in Figure 6 with additional imaging (CT, MRI) tailored to each patient. For instance, CT abdomen and pelvis should be obtained per general trauma guidelines, particularly if there is suspicion for solid organ or visceral injury.
![Figure 6: Elements of the Skeletal Survey. Although a full skeletal survey is currently the standard of care for patients with NAT, there are ongoing research efforts to tailor X-ray imaging more specifically to each patient. [1]](https://images.squarespace-cdn.com/content/v1/549b0d5fe4b031a76584e558/1570461092995-EBKSMB5DI0GTGXY0R75N/Figure+6%3A+Skeletal+surgery)
Figure 6: Elements of the Skeletal Survey. Although a full skeletal survey is currently the standard of care for patients with NAT, there are ongoing research efforts to tailor X-ray imaging more specifically to each patient. [1]
Other diagnoses to consider in these patients include metabolic bone disease (such as rickets, Caffey disease, and osteogenesis imperfecta), blood dyscrasias, benign enlarged subarachnoid spaces (BESS), glutaric aciduria type 1 (which causes brain atrophy and subdural fluid collections). [1] However NAT is far more common than these diagnoses and carries significant morbidity and mortality when overlooked so should be considered and worked-up prior to these diagnoses.
Key Points
Pediatric NAT causes significant morbidity and mortality, and therefore EPs must maintain a high degree of suspicion for this diagnosis.
Red flags during evaluation include a changing or inconsistent history, injuries inconsistent with the history, an unexpected mechanism of injury based on the child’s developmental status, and delayed presentation despite significant injury.
Risk factors for NAT include children younger than school age (with children younger than 1 being most vulnerable), family dysfunction, prematurity, multiple medical conditions, young/female parent, poor social support, unplanned or unwanted pregnancy, poor prenatal care, numerous separations from the child in the first year of life, and history of psychiatric issues, stressors, criminal activity, or childhood abuse or abandonment in the abuser.
Although physical exam findings can be non-existent or non-specific, highly specific findings include bruising over soft tissue areas; bruises/burns that are patterned take the form of an object; any bruising in a non-mobile child; scald burns on the hands, legs, feet, or buttocks; and stocking-and-glove patterned burns.
Highly concerning fracture patterns include classic metaphyseal lesions (“bucket handle fractures” or “corner fractures”), multiple posterior and/or lateral rib fractures, clavicular or spiral long bone fractures in any nonambulatory child, multiple fractures, fractures in different stages of healing, scapular fractures, sternal fractures, and spinous process fractures.
There is a wide range of ocular manifestations in NAT but the most common manifestation is retinal hemorrhage(s).
AHT carries the highest mortality rate of all the injuries associated with NAT. Any suspicion for AHT warrants consideration of a non-contrast head CT.
Notify Child Protective Services (CPS) and admit these children for further NAT work-up including a full skeletal survey.
Expert Commentary
Excellent overview of NAT in the Emergency Department with emphasis on risk factors and manifestations. I want to add a few pearls about NAT and then will focus my commentary on NAT management in the ED as well as discussion with families, as this was recently a large quality improvement project in our pediatric tertiary care center.
Neglect is the most common form of child abuse accounting for about two-thirds of all forms of abuse and often accompanies other forms of abuse. (1) Neglect is involved in about 50% of all cases of fatal child abuse. (1) Among children less than 1 year of age, 25% of fractures are a result of abuse. (2) Consider two things: does the explanation the provider stated account for the fracture the child has sustained? Is the child developmentally capable of the action being described? After 2 years of age, the history and physical exam should determine the imaging required. Over 5 years of age, the yield of unsuspected fractures from a skeletal survey is only 9%, making this group more amenable to selective radiographic studies. (3)
Diagnosis of NAT in children remains a challenge due to provider bias, preconceptions, and failure to recognize the presentation as possible abuse. (4,5) As a result, these injuries may go undetected, leading to further injury prior to diagnosis. An estimated 25% of children ultimately diagnosed with NAT have a sentinel injury prior to their abuse diagnosis. (6,7) Of abused children with a previous sentinel injury, the most common were a bruise (80%), a torn frenulum (11%), or a fracture (7%). (8) A large retrospective chart review estimated 80% of deaths from unrecognized abusive head trauma may have been prevented by earlier detection of NAT. (6) The American Academy of Pediatrics (AAP) states that “ANY injury to a young, pre-ambulatory infant” suggests abuse. (9)

Figure 1: Standardized Physical Abuse Guideline.
At our institution, a team of pediatric emergency medicine physicians and child abuse pediatricians convened to develop and implement a standardized NAT guideline for providers in the ED when evaluating children with suspected NAT (Figure 1 Standardized Physical Abuse Guideline). This work stemmed from a chart review showing there was significant variability in the evaluation and management of children with concern for NAT in our Pediatric Emergency Department. The guideline was based on current peer reviewed literature as well as local expert consensus. It is divided into three separate age groups: < 6 months, 6-12 months, and >12-36 months. Age groups were determined based on risk of injury at different age levels in described literature, acquisition of milestones as age progresses, and increased ability for young children to show specific signs of injury with increasing age.
Lastly, the evaluation of NAT is stressful for both families and healthcare providers. The second page of our NAT guideline gives a sample script for EPs when discussing the non-accidental trauma evaluation for children. It states, “Any time a child comes to the hospital with this injury/these injuries, we evaluate for other injuries. Sometimes a child can have internal injuries such as fractures, head injury or abdominal injuries that we cannot see on the outside. Just like you, we want to make sure that your child is okay, so it is important to do this testing. We will also have our social worker come talk to you. This is a standard part of our evaluation. We are happy to answer any questions along the way”. It is important to acknowledge that this process is stressful, time consuming, and not comfortable for the child. Explaining each part of the process is important. Ensure that you use language that is non-accusatory. As EPs, we are not the ones to identify who the perpetrator is/was, but rather ensure the full NAT evaluation is completed and allow social work and/or Child Protective Services to determine further action.
Non-accidental trauma remains too prevalent in our country. Literature continues to show that unrecognized NAT leads to worse injuries and sometimes fatality. Continuing knowledge and education about injuries suspicious for NAT for EPs remains imperative. Standardized evaluations and real time order sets can increase appropriate management of NAT in the Emergency Department.
References:
Dubowitz H. Epidemiology of Child Neglect. CAN 2011, pp 28-34.
Kaczor K, Clyde Pierce M. Abusive Fractures. CAN 2011, pp 275-295.
Martich KV. Imaging of Skeletal Trauma in Abused Children. CAN 2011, pp 296-308.
Higginbotham N, Lawson KA, Gettig K, et al. Utility of a child abuse screening guideline in an urban pediatric emergency department. J Trauma Acute Care Surg. 2014;76(3):871-877.
Tiyyagura GK, Gawel M, Koziel JR, et al. Barriers and facilitators to detecting child abuse and neglect in general emergency departments. Annals of Emergency Medicine. 2015;66(5):447-454.
Jenny C, Hymel K, Ritzen A, et al. Analysis of missed cases of abusive cases of head trauma. JAMA. 1999;282:621-6.
Rangel EL, Cook BS, Bennett BL, et al. Eliminating disparity in evaluation for abuse in infants with head injury: use of a screening guideline. Journal of Pediatric Surgery. 2009; 44(6):1229-34.
Sheets LK, et al. Injuries in Infants Evaluated for Child Physical Abuse. Pediatrics. 2013, pp 701-707.
Christian CW, Committee on Child Abuse and Neglect. The evaluation of suspected child physical abuse. Pediatrics. 2015;135:e1337–e1354.

Lauren C. Riney, DO
Assistant Professor
Division of Emergency Medicine
UC Department of Pediatrics
How to Cite this Post
[Peer-Reviewed, Web Publication] Loke D, Amick A. (2019, Oct 7). Non-Accidental Trauma. [NUEM Blog. Expert Commentary by Riney C]. Retrieved from http://www.nuemblog.com/blog/nonaccidental-trauma.
Other Posts You Might Enjoy
References
Pfeifer, C.M., Hammer, M.R., Mangona, K.L., & Booth, T.N. (2017). Non-accidental trauma: the role of radiology. Emerg Radiol, 24, 207-213.
Kim, P.T. & Falcone, R.A. (2017). Non-accidental trauma in pediatric surgery. Surgical Clinics of North America, 97.1, 21-33.
Child maltreatment 2014. Report, Children’s Bureau. Washington, DC: U.S. Department of Health and Human Services; 2014. Available at: http://www.acf. hhs.gov/sites/default/files/cb/cm2014
Paul, A.R. & Adamo, M.A. (2014). Non-accidental trauma in pediatric patients: a review of epidemiology, pathophysiology, diagnosis and treatment. Transl Pediatr, 3, 195-207.
Maguire, S., Mann, M.K., Sibert, J. & Kemp, A. (2005). Are there patterns of bruising in childhood which are diagnostic or suggestive of abuse? A systematic review. Arch Dis Child, 90, 182-186.
Boos, S.C. (2017). Physical child abuse: Recognition. Retrieved April 21, 2017, from http://www.uptodate.com
Hobbs, C.J. (1986). When are burns not accidental? Archives of Disease in Childhood, 61, 357-361.
Binenbaum G., Rogers, D.L., Forbes, B.J., Levin, A.V., Clark, S.A., Christian C.W., Liu, G.T., & Avery R. (2013). Patterns of retinal hemorrhage associated with increased intracranial pressure in children. Pediatrics, 132, 430-434.
Litz, C.N., Ciesla, D.J., Danielson, P.D. & Chandler, N.M. (2017). A closer look at non-accidental trauma: Caregiver assault compared to non-caregiver assault. Journal of Pediatric Surgery, 52, 625-627.
Pediatric ECMO: Beyond the Basics of Pediatric Resuscitation
Written by: Steve Chukwulebe, MD (NUEM PGY-4) Edited by: Spenser Lang, MD (NUEM ‘17) Expert commentary by: Leah Harris, MD and Kiona Allen, MD
Case
A 38-year-old G8P6 female at 39-weeks gestation presents to your emergency department in active labor. The patient has gotten all her prenatal care at your institution, but has not made it to her due date. She reports her water breaking about 2 hours ago. She describes that the ruptured fluid was not clear but dark yellow/green, and she is now experiencing contractions every 2 minutes.
Your bedside doppler reveals reassuring fetal heart tones at a rate of 152. On your initial exam, the cervix is fully dilated and effaced…and you see the baby’s head. As your obstetric colleagues are several minutes away, you check your pulse, dust off the radiant warmer, and prepare your resources for an ED delivery.
The mother delivers within the next few minutes with your OB colleagues still en-route. While she has minimal complications, the newborn is now not doing as well.
Neonatal Exam
Constitutional: Full term boy, covered in meconium
Skin: Appears blue gray, cool to touch
Respirations: For the most part apneic and at times grunting
CV: Heart rate 100
Tone: Flaccid
You take over the resuscitation of the neonate immediately as he is delivered given the above exam. Attempts at stimulation, drying, oral suctioning, and warming still yields a 1-minute APGAR of 3.
NRP/PALS
As per the algorithm below, with continued apnea and SpO2 in the 50’s you begin positive pressure ventilation and continued stimulation [1]. At 15 minutes, despite your attempts with continued PPV, suctioning, and stimulations, the SpO2 continues to be in the 60’s and the heart rate begins trending towards from 100 to the 60’s as well. You decide to intubate the patient, and the tube is passed successfully. Tube placement is confirmed and the x-ray shows fluffy infiltrates bilaterally in both lung fields but no evidence of barotrauma. Attempts at bagging yields minimal resistance, however the highest SpO2 the patient reaches is in the low 80’s at 40 minutes, with improved heart rate to the 120’s. At this point, your pediatric colleagues have found their way to the ED and are ready to take the neonate to the NICU. Two hours later into your shift, you read that the neonate was placed on veno-venous extracorporeal membrane oxygenation (ECMO) and is doing better. After your shift is over, you find your way over to the NICU and you see a pink sedated baby under a radiant warmer and connected to a large ECMO circuit.
Diagnosis: meconium aspiration syndrome complicated by pulmonary vascular hemorrhage and ARDS.

Had this neonate been in your ED, and your resuscitative measures have been exhausted, at what point do you consider ECMO in the neonatal or pediatric patient? I will review briefly the emergence of ECMO in the neonatal and pediatric literature, as well as its indications and the limited data on its utility in the emergency department setting.
From theory to practice
The first cardiac bypass circuit was created by John Gibbon in 1936 in the operating suite. ECMO is defined as a mechanical circuit outside the body where blood oxygenation and carbon dioxide removal can occur for patients with reversible cardiac or respiratory failure [2]. Through the 1950-1970s, many researchers studied various materials and techniques to further improve membrane oxygenation and attempted to increase the length of time a patient could remain on bypass. However, it was not until 1976 in which Bartlett et al. reported on the first neonate suffering from meconium aspiration syndrome to be successfully treated ECMO [3]. Since then, ECMO has grown and been used in various forms as treatment of respiratory failure in the neonatal and pediatric ICU settings. ECMO is to be considered for any reversible pathologic process that is impeding adequate tissue oxygenation and ventilation.
Indications for ECMO in children
Neonates:
Primary pulmonary hypertension of the newborn
Meconium aspiration syndrome
Persistent fetal circulation
Congenital diaphragmatic hernia
Pediatrics:
Respiratory failure
Bronchiolitis
RSV
Pneumonia
ARDS
Aspiration
Status asthmaticus
Sepsis
Cardiac arrest
with reversible conditions or amenable to heart transplantation
with favorable neurologic outcomes, some studies show better outcomes with CPR initiated in up to 95 minutes [5], key being excellent CPR with ETCO2 > 10 and early recognition and initiation of eCPR (extracorporeal cardiopulmonary resuscitation)
Hypothermia (cold water drowning)
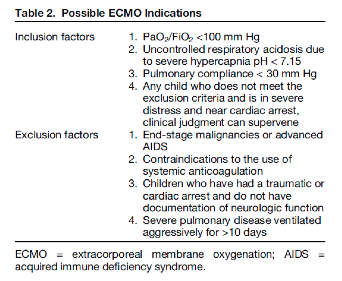
In general, pediatric ECMO has been found useful in the above settings, however Gehrmann et al. reviewed the indications across various institutions when patients have been refractory to medical therapies. These indications are shown in the table below.
Types
ECMO comes in two types: venoarterial (VA) and venovenous (VV). While the early VA ECMO circuits utilized the roller pump to provide non-pulsatile flow of oxygenated blood, its limitations for infants included the necessity to cannulate the artery via either an open sternotomy or open cannulation of the carotids with the risk of losing a unilateral carotid artery due to ligation [4]. VV ECMO is the newer of the two modalities and rather than accessing a major vein and a major artery, the circuit requires access to either 2 major veins or a single major vein using a double-lumen catheter. However, each modality has its associated risks and benefits as described in the chart below [2].

Outcome Data
Neonates:
Neonates generally have better survival and outcomes on ECMO than older children and adults. One single center retrospective study in the journal of pediatric critical care published that of the 264 neonates placed on ECMO, 211 (80%) survived to discharge and 10-year survival was 71% [5]. The study had 2 cohorts and followed both neonatal and pediatric patients, collecting both demographic and survival data from patients placed on ECMO from 1987 to December 2013. Of those neonates that were alive at 90 days, at a 10-year follow up (ie.10-year conditional survival) 93% were alive. Of the common indications for neonatal ECMO, the 90-day survival and 10-year conditional survival are as follows respectively:
meconium aspiration syndrome (99% and 100%)
congenital heart anomalies (58% and 86%)
congenital diaphragmatic hernia (68% and 74%)
neonatal infection (72% and 100%)
Furthermore, patients who underwent VV ECMO had better 90-day survival and 10-year conditional survival rates than VA ECMO, 92% vs. 69%, and 98% vs. 87% respectively.
Pediatrics:
The same study followed 136 pediatric patients as well showing that the 90-day survival rate was 66% (90 patients) and that the 10-year conditional survival rate was 89%. The study divides the 90-day survival rates for ECMO by splitting it between pneumonia (bacterial, viral, and aspiration, 66, 76, and 83% respectively), other causes of sepsis (33%), trauma (100%), and other respiratory etiology (63%). Again, patients who underwent VV ECMO had better 90-day survival rates than VA ECMO, 78% vs. 50% respectively.
Other retrospective studies report similar survival rates to discharge when ECMO is used for severe respiratory failure, with rates from 39% to 83% depending on the pulmonary diagnosis, with status asthmaticus having survival rates of 83-100% on ECMO [2,6].
Data in ED
While data on emergency department utilization of pediatric ECMO is limited, one study mentions the outcomes from its two cases [7]. The first case was a 3-year-old previously healthy girl who presented with nausea and developed cardiogenic shock in the department from viral myocarditis. This patient was placed on ECMO in the ED and transferred to the cardiac intensive care unit. She was taken off the circuit after 4 days with improved contractility, and eventually discharged home 10 days later neurologically intact. The second case was similar in etiology: a 17-year-old male who presented in respiratory distress and suffered a PEA arrest. This patient achieved ROSC, was placed on ECMO in the ED and was eventually discharged home 31 days later with a favorable neurological outcome.
Conclusions
While some centers continue to grow their extracorporeal membrane oxygenation programs to expand their resuscitative efforts, still few places have the equipment to start the circuit or even at times an on-call staff to prime the machine. In general, few studies report the usage of ECMO in the emergency departments as a means for cardiopulmonary resuscitation of a reversible etiology, and only case reports exist in the pediatric literature. However, even if the ability to start neonatal/pediatric ECMO may not be ever be present in one’s emergency department, prompt recognition and early disposition to tertiary care centers that offer these services could potentially be lifesaving in many appropriate cases.
Expert Commentary
While ECMO (extracorporeal membrane oxygenation) may seem a foreign concept for ED management, it is important to recognize that as recently as the 2009 H1N1 epidemic, utilizing this intervention as a rescue therapy to treat acute severe hypoxic respiratory failure associated with influenza resulted in cases of ECMO initiation in emergency rooms across the world. Your review introduces meconium aspiration – a frequent clinical indication – as a platform to review this technology. Critical to the understanding of ECMO is first to be able to determine the appropriate candidates for this support, then to pick the correct mode (veno-arterial versus veno-veno) and to learn your own institution’s interpretations of inclusion and exclusion criteria. For the purposes of this commentary, we will break down the review into five sections sections: types of ECMO, who goes on ECMO, how to measure and trend hypoxemia, what can you do in the ED to maximize success on ECMO and new advances in ECMO.
ECMO modes:
ECMO is temporary cardiopulmonary bypass used to support a patient with either heart or lung failure. Originally developed from modifications of cardiopulmonary bypass and subsequently adapted for prolonged support, an ECMO circuit has both an oxygenator and a pump and a rate by which the blood passes across the oxygenator filter and has carbon dioxide removed. Children with heart or lung failure who do not respond to conventional medical therapies may be candidates for ECMO support. The ECMO circuit drains blood from the body, exchanges oxygen and carbon dioxide on the red blood cell, warms the blood and pumps it back into the body. Placing a child on ECMO allows time for the heart and/or lungs to improve or to serve as a bridge to other long-term extracorporeal support or transplant.

In this very simple model, the oxygenator functions as the lungs, the pump takes over the work of a beating heart and the flow of the blood across the oxygenator mimics a respiratory rate and removes the carbon dioxide. If a patient’s heart is still adequately functioning as a pump and the indications for ECMO are due to oxygenation and/or ventilation defects, then utilizing ECMO as an isolated pulmonary bypass is preferred and veno-venous cannulation is warranted. Blood is therefore removed from a vein, red blood cells are oxygenated and carbon dioxide removed, and then blood is returned to a vein for the heart to pump. This approach allows for an adequate mixed venous saturation and tissue oxygenation. More importantly it allows for the heart to perfuse the coronary arteries with antegrade flow, does not require that an artery be sacrificed for access, permits a pulsatile waveform to be sensed by organs and can often be performed with a single dual-lumen catheter. Most frequent sites are internal jugular vein or femoral vein. Cannulation can be accomplished by either using 2 separate cannulae or by utilizing a dual lumen internal jugular cannula that spans from superior vena cava (SVC) to inferior vena cava (IVC) in order to remove blood via end and side ports in the cavae and return blood via a side port of the second lumen that is positioned in the right atrium and directed towards the tricuspid valve.

If the patient has had any indications of cardiac injury including but not limited to cardiac arrest, arrhythmias, severe pulmonary hypertension, or evidence of significant cardiac dysfunction, then venoarterial cannulation is indicated as the patient’s heart can no longer be relied upon to pump blood.
ECMO Candidates:
The review elegantly lists criteria for candidacy but there are few others to be considered including mediastinal masses with airway compression and complex airway disease. Usually ECMO is on stand-by for these cases in the operating room.

Measurement of hypoxemia:
While many are using P/F ratio (as Steve commented on in his review), the gold standard remains calculating and trending oxygenation index as a surrogate marker for severity of hypoxemia. Patients with an OI > 25 x 6 hours are demonstrating refractory severe lung failure and should be considered for ECMO.

Pre-ECMO Studies:
If you have a patient scenario develop in the Emergency Department with a high likelihood of progression to ECMO, there are handful of tests/treatments to be ordered prior to initiating ECMO that will make the decision to proceed with ECMO easier for the inpatient team:
1. Is there any evidence of a CNS abnormality or bleed? Order a head ultrasound on the infant or a head CT on the child if able – you want to rule out any CNS bleed that would be worsened by anti-coagulation.
2. Does the child have an underlying congenital heart lesion? Order an ECG and ECHO on every patient – you want to rule out any congenital cardiac lesions and to quantify pulmonary hypertension.
3. Is there any evidence of pulmonary hypertension – regardless of whether this is acquired or idiopathic? If “yes” – then start iNO – you can presume that all mechanisms of respiratory failure are coupled with worsening pulmonary hypertension in the child.
4. Order a type and screen and a CBC. While not ideal, a baby with a hemoglobin of 14 g/dL can be placed on a saline-primed ECMO circuit emergently with the recognition that this will dilute and drop their Hg and interfere with oxygen carrying capacity. For smaller children where the total volume of the ECMO circuit can exceed their own intravascular volume, best to be able to prime the ECMO circuit with blood before placing the patient on the ECMO pump.
New Advances in ECMO:
The ECMO world is pushing the envelope and recognizing that preventing deconditioning and minimizing de-recruitment of both lung tissue and muscle mass is key to recovery or to eventual organ transplantation. Centers across the US and Europe now have their patients walking on ECMO. Who knows, one may walk into an ER near you some day!!

Kiona Allen, MD
Assistant Professor of Pediatrics, Cardiology

Leah Harris, MD
Professor of Pediatrics, Pediatric Clinical Care
How To Cite This Post
[Peer-Reviewed, Web Publication] Chukwulebe S, Lang S. (2019, April 8). Pediatric ECMO: Beyond the basics of pediatric resuscitation [NUEM Blog. Expert Commentary by Harris L & Allen K]. Retrieved from http://www.nuemblog.com/blog/pediatric-ecmo
Other Posts You May Enjoy
Resources
Pediatrics AA, Association AH. Textbook of neonatal resuscitation. 2006.
Gehrmann LP, Hafner JW, Montgomery DL, Buckley KW, Fortuna RS. Pediatric Extracorporeal Membrane Oxygenation: An Introduction for Emergency Medicine Physicians. J Emerg Med. 2015;49(4):552-60.
Bartlett RH, Gazzaniga AB, Jefferies MR, Huxtable RF, Haiduc NJ, Fong SW. Extracorporeal membrane oxygenation (ECMO) cardiopulmonary support in infancy. Trans Am Soc Artif Intern Organs 1976;22:80—93.
Mok YH, Lee JH, Cheifetz IM. Neonatal Extracorporeal Membrane Oxygenation: Update on Management Strategies and Long-Term Outcomes. Adv Neonatal Care. 2016;16(1):26-36.
Alsoufi B, Osman A, Nazer R, et al. Survival outcomes after rescue extracorporeal cardiopulmonary resuscitation in pediatric patients with refractory cardiac arrest. J Thorac Cardiovasc Surg 2007; 134:952–9.
Swaniker F, Kolla S, Moler F, et al. Extracorporeal life support outcome for 128 pediatric patients with respiratory failure. J Pediatr Surg. 2000;35(2):197-202.
Nevet A, Polak T, Dagan O, Waisman Y. Extracorporeal Membrane Oxygenation as a Resuscitation Measure in the Pediatric Emergency Department. Isr Med Assoc J. 2015;17(10):639-41.
Infantile Colic
Most infants cry more during the first three months of life than at any other time. As an emergency medicine physician, it’s crucial to rule out other etiologies of fussiness before discharging with pediatrician follow up. You can find some tips and tricks here to help you with this difficult diagnosis in the emergency department.
Neonatal Sepsis: A Brief Visual Guide
Mitali Parmar makes understanding neonatal sepsis ridiculously simple with visual guide to this uncommon but cannot miss diagnosis.
Steroid Selection In Pediatric Asthma
Pediatric asthma exacerbations account for a significant portion of trips to the emergency department (ED), comprising 2-4.5% of ED visits each year. As a common disease of the pediatric population, effective ED management is key. The current mainstay of treatment is beta-agonist and corticosteroid administration. Here we discuss the evidence behind steroid selection in the pediatric asthmatic presenting to the emergency department.