Written by: Mitchell Blenden, MD (NUEM ‘24) Edited by: Em Wessling (NUEM ‘22) Expert Commentary by: Tim Loftus, MD, MBA


Expert Commentary
Thank you to Dr’s Blenden and Wessling for the excellent overview of ED CDUs including some background and indications for their use.
Several points to highlight and elaborate upon include the following:
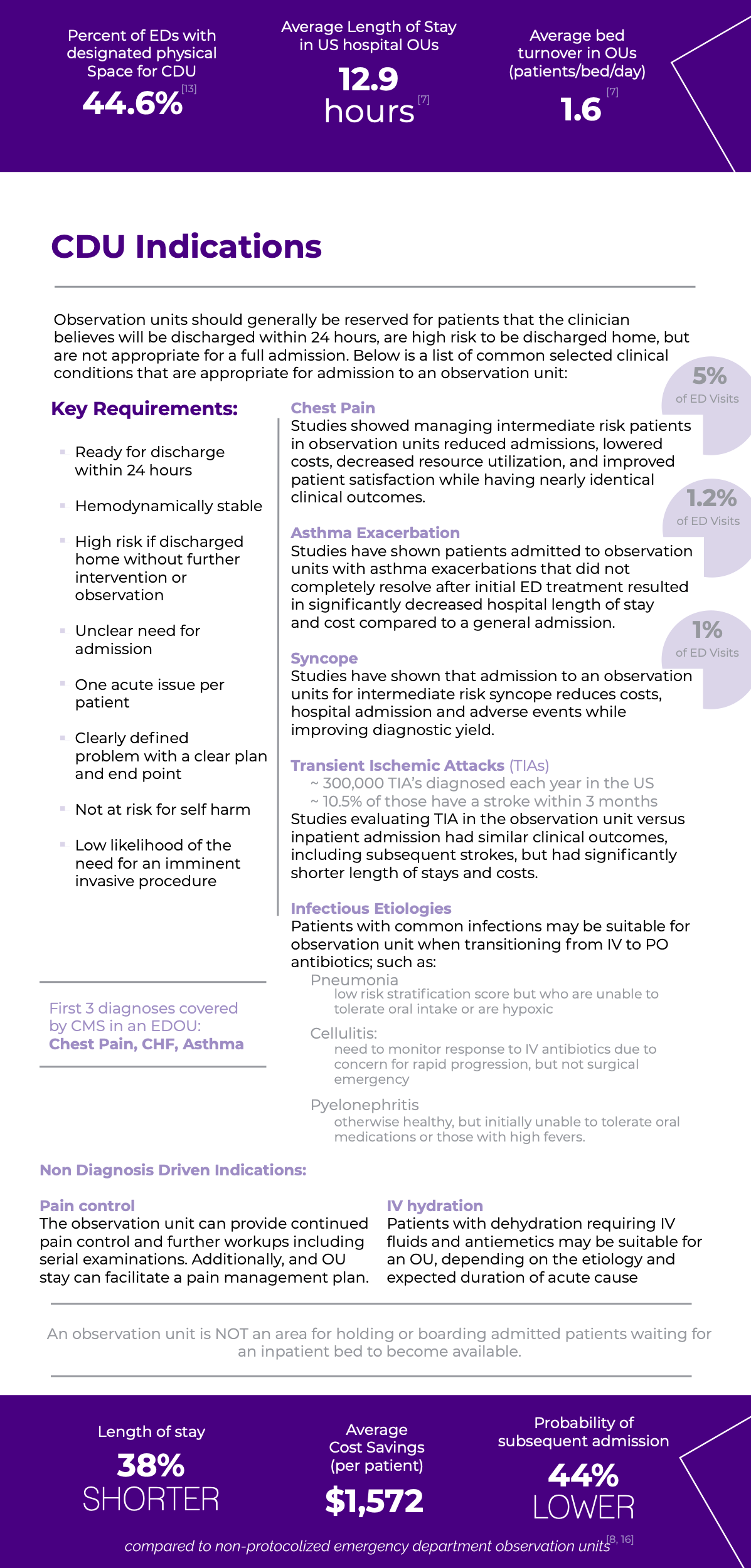
The background of the utility of CDUs mostly stems from their early function as rapid diagnostic and treatment centers (RDTCs) for chest pain. The function and utility of CDUs have since grown to demonstrate clinical benefits well-established across a variety of conditions as Dr’s Blenden and Wessling have mentioned, including not only chest pain (rule out acute coronary syndrome) but also TIA, CHF, asthma, COPD, cellulitis, pyelonephritis, pneumonia, etc.
Value and Benefits
The utility and value of ED CDUs will continue to expand. The percentage of all hospital admissions that start in the ED continues to grow -- 67% in 2019, up from 58% in 2004 according to the ED Benchmarking Alliance. Additionally, EDs cared for approximately 158M people as of 2018 (EMNet/NEDI-USA), up 32% over a 10 year period. As the number of admissions continues to grow, and considering that some of these inpatient stays are short, it follows that many of these short inpatient admissions are subject to recovery audit contractors and payor denials. Many clinical conditions which are often subject to short inpatient stays can be cared for in dedicated short stay observation units without adversely affecting, and for the most part improving, the quality of care delivery, safety, satisfaction, cost savings, and reducing subsequent inpatient LOS.
All stakeholders in the health care system benefit from CDU use: patients are more accurately diagnosed before leaving the ED and are discharged home faster, payors avoid costly inpatient admission charges, hospitals keep scarce inpatient bed capacity open for more appropriate patients and avoid audits and denials, and providers deliver care in a setting that more appropriately matches patient needs to resources.
Dedicated Units with Protocolized Care
Observation patients can be managed in a variety of settings and contexts, but best practice that leads to best outcomes would be in dedicated observation units adherent to protocols tailored to the patients’ conditions, the best available evidence, and local institutional resources.
Shorter hospitalizations are more likely to occur in dedicated observation units under protocols than with unstructured hospitalization on inpatient teams and simply billing status changes to observation.
Financial Considerations
Much of the existing evidence has demonstrated that CDUs can provide care that efficiently utilizes resources and results in shorter hospital lengths of stay relative to other projects to expand capacity. Further, hospitals may realize decreased operating expenses for those patients subsequently discharged home from the CDU who have diagnoses or clinical conditions that are not as profitable for the hospital to manage in the inpatient setting - for example, CHF, which can often create a loss for the hospital. That being said, hospitals should be careful about shifting too much acute care into CDUs, because any CDU stay that subsequently results in inpatient admission (about 20% or so) are only paid by a single DRG, which includes that care provided for in the ED, CDU, and hospital unit. Thus, you can risk incurring additional costs without additional revenue. Finally, the duration of observation should exceed 8 hours only to justify the added expense of operating the CDU, because payors, including Medicare, generally do not pay clinical or facility fees for observation stays less than 8 hours.
Another consideration when estimating value created by a CDU is the increasing use by those who would have otherwise been discharged from the ED. It is important to consider the value of a CDU not only by the cost savings to the hospital and patient but also the possible supply-induced demand of health care services and overutilization of those services to a detriment.
CMS, and other payors, do not necessarily exclude payment from observation status patients whose stay lasted longer than 24 or even 48 hours. However, the profit margin and efficiency are reduced when patients are staying in the CDU that long, highlighting an opportunity to evaluate your particular unit’s effectiveness, efficiency, and patient selection.
Final Considerations
CDUs are not appropriate for all EDs, as only about 5-10% of ED patients have been found to be appropriate for a CDU, and in order to optimize operational and financial efficiency, a certain minimum number of beds and fixed costs would need to be overcome.
It is worth mentioning that protocol-driven CDUs in proximity to an ED with dedicated diagnostic and treatment algorithms, patient selection criteria, predetermined outcomes and end points have demonstrated the best outcomes with respect to cost savings, patient satisfaction, safety, and reduction in hospital LOS. For administrative and clinical operations leaders, tracking process and outcome metrics such as LOS, occupancy rate, discharge rate, and bed turns in addition to other clinical and quality outcomes will enable ongoing continuous optimization of the CDU.
Depending on the resources and throughout considerations of each hospital and health system, at times CDUs provide great benefit in being able to flexibly accommodate inpatient holds, pre or postoperative patients, or additional acute ED treatment space as the need allows. Design and construction with this in mind may enable the hospital to best accommodate ever changing dynamics - COVID being one example.
References
Emergency Medicine Network (EMNet). National Emergency Department Inventory – USA. https://www.emnet-usa.org/research/studies/nedi/nedi2018/. Accessed 1 Jan 2021.
Emergency Department Benchmarking Alliance (EDBA). Before there was COVID - 2019 Emergency Department Performance Measures Report. Accessed 1 Jan 2021.
Baugh CW, Liang L-J, Probst MA, Sun BC. National Cost Savings From Observation Unit Management of Syncope. Academic Emergency Medicine. 2015;22(8):934-941. doi: 10.1111/acem.12720.
Baugh, C. W., Venkatesh, A. K., & Bohan, J. S. (2011). Emergency department observation units: a clinical and financial benefit for hospitals. Health care management review, 36(1), 28-37.
Baugh and Granovsky - ACEP Now - https://www.acepnow.com/article/new-cms-rules-introduce-bundled-payments-for-observation-care/?singlepage=1
Making Greater Use Of Dedicated Hospital Observation Units For Many Short-Stay Patients Could Save $3.1 Billion A Year. Health Affairs. 2012;31(10):2314-2323. doi: 10.1377/hlthaff.2011.0926.
Ross MA, Hockenberry JM, Mutter R, Barrett M, Wheatley M, Pitts SR. Protocol-driven emergency department observation units offer savings, shorter stays, and reduced admissions. Health Aff (Millwood). 2013;32(12):2149-2156. doi: 10.1377/hlthaff.2013.0662.
Rydman RJ, Zalenski RJ, Roberts RR, et al. Patient satisfaction with an emergency department chest pain observation unit. Ann Emerg Med. 1997;29(1):109-115. doi: 10.1016/s0196-0644(97)70316-0.

Timothy Loftus, MD, MBA
Assistant Professor
Department of Emergency Medicine
Northwestern University
How To Cite This Post:
[Peer-Reviewed, Web Publication] Blenden, M. Wessling, E. (2021, Apr 12). ED Clinical Decision Making Units. [NUEM Blog. Expert Commentary by Loftus, T]. Retrieved from http://www.nuemblog.com/blog/ed-clinical-decision-making-units.