

Written by: Priyanka Sista, MD (NUEM PGY-4) Edited by: Matt Klein, MD (NUEM ‘18) Expert commentary by: Shannon Lovett, MD
Expert Commentary
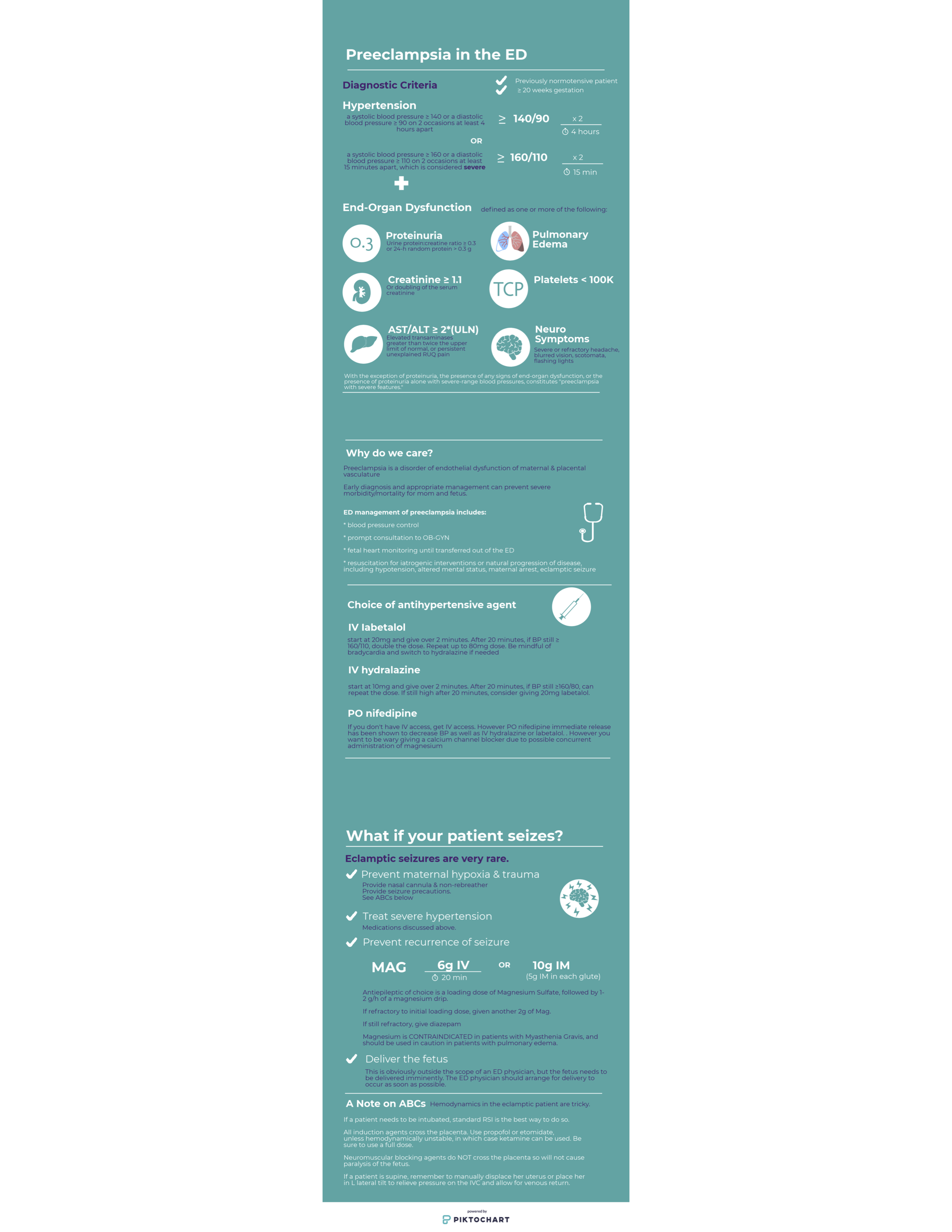
Thank you for this succinct guide to the diagnosis and management of preeclampsia in the ED.
“The eyes do not see what the mind does not know…..”. The biggest pitfall in the management of preeclampsia in the ED, is failing to consider and recognize the diagnosis. Recognition and prompt treatment of preeclampsia in the ED setting can be challenging due to the variety of presenting complaints. It is important to note that preeclampsia may occur anytime from 20 weeks gestation up to 6 weeks postpartum.
Postpartum preeclampsia tends to be more diagnostically challenging and depending on your facility, these patients are more likely to present to the ED than pregnant patients who often present to their obstetrician or to labor and delivery. Preeclampsia in the postpartum period most frequently occurs in the first 48 hours after delivery, but should be considered up to 6 weeks postpartum. Patients with postpartum preeclampsia often do not have hypertensive disease or preeclampsia during pregnancy.
The complaints associated with preeclampsia may be broad and vague- including but not limited to: headache, vision changes, swelling or rapid weight gain, nausea and vomiting, shortness of breath, and abdominal pain. Consider preeclampsia or eclampsia in the critical female patient that arrives in the ED with little known history- for example actively seizing, or in respiratory distress with pulmonary edema.
The treatment of preeclampsia can be broken down into three parts: treating the hypertension, reducing the risk or recurrence of seizures, and delivery of the fetus and the placenta. In the ED- our focus is on the first two, and involving our obstetric colleagues immediately. Blood pressure is most commonly treated with labetolol or hydralazine IV in the ED, and Mag should be given immediately for seizure prophylaxis (or to reduce recurrence of seizures in eclampsia).
Lastly, our obstetric and gynecology colleagues at ACOG have recognized the frequency that postpartum patients present to the ED, and have created this ED checklist that can be used as a reference for the management of postpartum preeclampsia- https://www.acog.org/-/media/Districts/District-II/Public/SMI/v2/19sm03a170703PPPreeclamCheckED1.pdf?dmc=1&ts=20190327T1949153065. Preeclampsia is a syndrome with potentially devastating consequences to mother and baby, and our early recognition and treatment can improve outcomes.

Shannon Lovett, MD
Associate Professor
Loyola University Medical Center
How To Cite This Post
[Peer-Reviewed, Web Publication] Sista P, Klein M. (2019, Sept 23). Preeclampsia. [NUEM Blog. Expert Commentary by Lovett S]. Retrieved from http://www.nuemblog.com/blog/preeclampsia.
Other Posts You May Enjoy







The author underscores the central position the emergency provider may hold in identifying and supporting victims of trafficking