

Written by: Ziggy Uvin MD (NUEM ‘28) Edited by: Tori Adomshick, MD (NUEM ‘27)
Expert Commentary by: Amer Aldeen, MD (USACS)
Expert Commentary
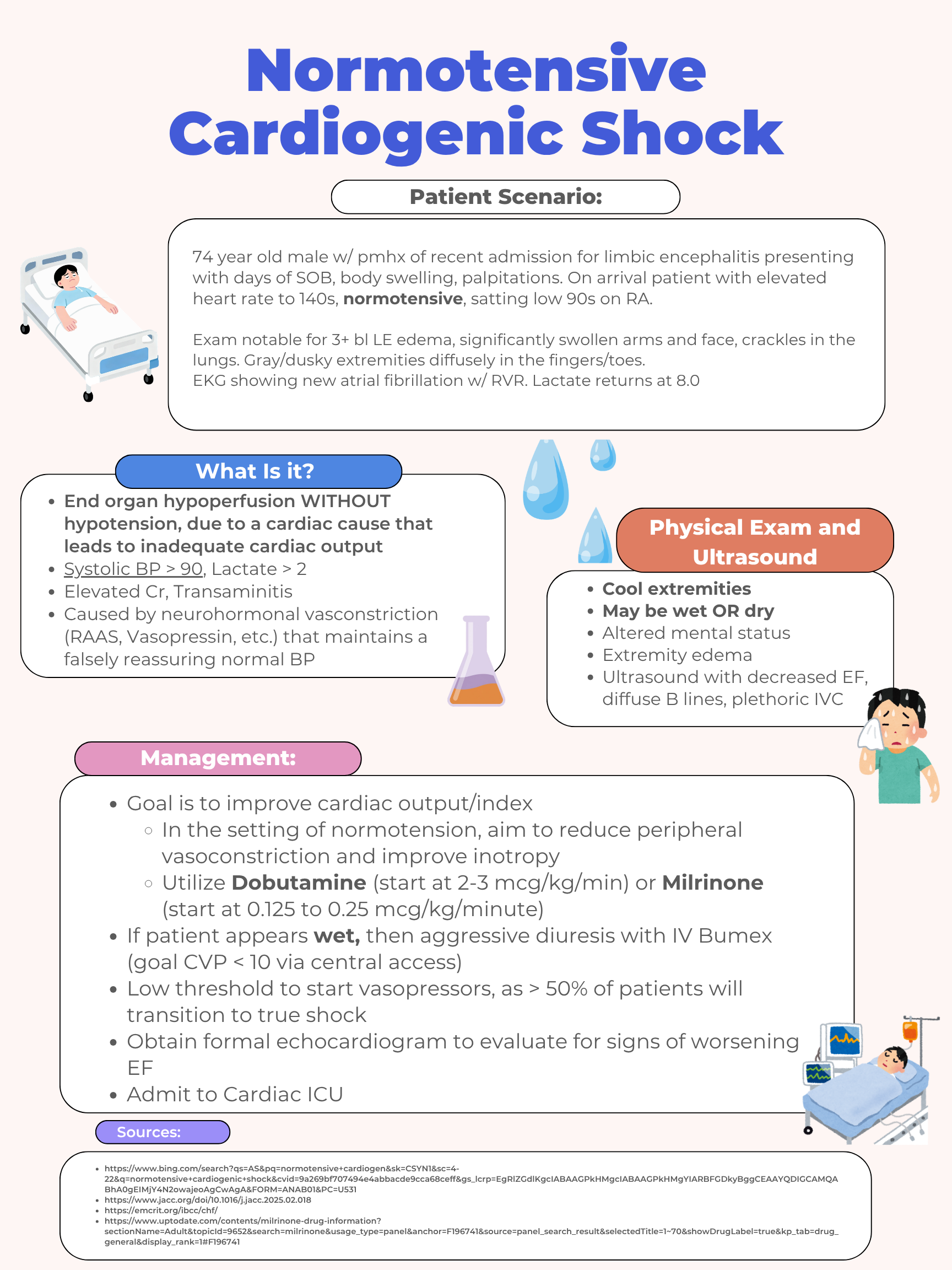
74-year-old male with dyspnea, edema, and palpitations, HR 140s, low 90s% SpO2. But the BP is normal, so he’s not in shock, right?

Dr. Amer Aldeen, MD, FACEP
Chief Transformation Officer and Chief Medical Officer
US Acute Care Solutions
Of course, we know this is wrong. Not all shock exhibits hypotension—in fact, mortality from hypoperfusion without hypotension may be higher than from hypotension without hypoperfusion (Jentzer 2021). The physical exam reveals shock with poorly perfused extremities, a lactate of 8.0, and an EKG showing presumably new atrial fibrillation, which basically reflects critical illness. You can also use the shock index (HR/sBP) for a quick check—if shock index >1, you could be dealing with shock, even if your BP is normal.
While the exam reveals clear elements of cardiogenic shock, one cannot yet rule out septic shock as the alternative or additional diagnosis. Remember that geriatric patients don’t exhibit fever or leukocytosis as often as non-geriatric adults do. For this reason, I’d add to this evaluation broad spectrum antibiotics until you have comfortably excluded septic shock.
In addition to the loop diuretic, dobutamine/milrinone, and echo, make sure you assess emergently addressable reasons for cardiogenic shock—check for MI with troponin and use U/S to check the pericardium.
How To Cite This Post:
[Peer-Reviewed, Web Publication] Uvin, Z. Adomshick, T. (2026, July 5). Normotensive Cardiogenic Shock [NUEM Blog. Expert Commentary by Aldeen, Ameer]. Retrieved from http://www.nuemblog.com/blog/normotensivecardiogenicshock.









