

Written by: Zain Khawaja, MD (NUEM ‘29) Edited by: Dean Hayes, MD (NUEM ‘27)
Expert Commentary by: Seth Trueger, MD (NUEM)
Expert Commentary

Thank you Dr. Khawaja and Hayes for this nice overview of the ECG in syncope. Syncope management can be frustrating: syncope can be pretty scary for patients and their family and friends, yet only a small fraction of patients with syncope are at risk for bad outcomes; and, unfortunately our ability to identify who is at higher risk is not very accurate, probably because so many different things can lead to syncope. The overall approach to syncope—eg, syncope vs seizure, no brain imaging without concerns for SAH or trauma, treating near or pre-syncope the same as syncope—is summarized well by Anton Helman in ACEP Now(1); I also find the now older 2007 ACEP Clinical Policy on syncope informative and surprisingly readable.(2)
Briefly, before getting into ECG specifics, my approach is to think first about higher risk HPI features (eg, exertional syncope, lack of or absent prodrome), higher risk PMH features (eg, older age, structural heart disease, known coronary artery disease, or heart failure – heart failure causes VT, hence common ICD placement in people with heart failure). The 2007 ACEP paper also suggests anemia is a risk factor in some models; I use this as a reminder to think about ruptured AAA and GI bleeds.
My approach to the ECG in syncope is to start with the more obvious: is there ischemia or blocks? Specifically, is there a high-grade AV block (Mobitz 2 or complete heart block), or poorly named “trifascicular block,” which can be a few things: a right bundle branch block plus an LAFB or LBFB (ie, half of a left bundle branch block) plus a first degree AV block(3); alternating RBBB & LBBB, or RBBB plus alternating LAFB/LPFB.(4) A trifascicular block can indicate impending complete heart block; in the setting of syncope, it is concerning enough to admit and consult EP or cardiology.
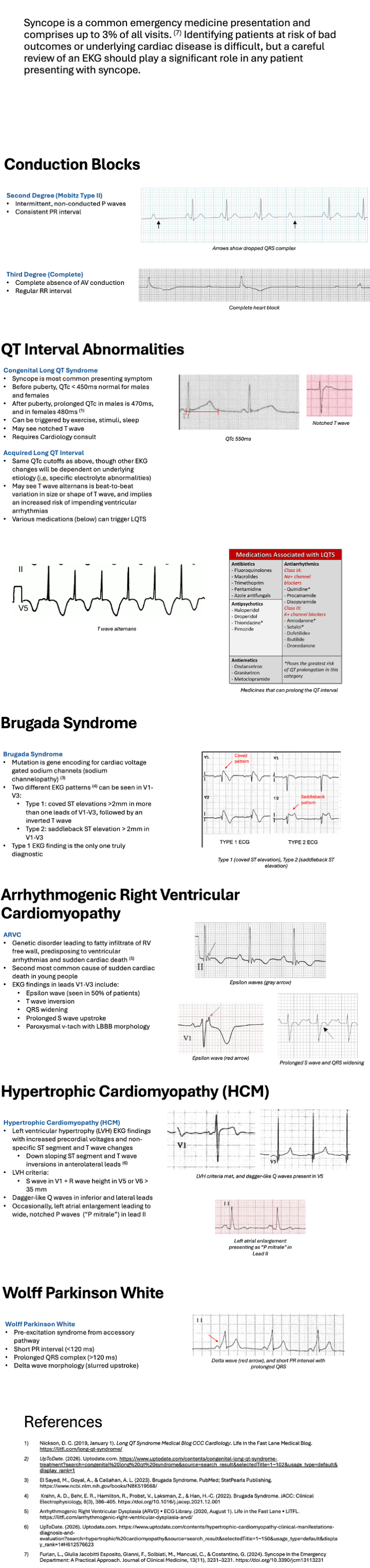
The last part is the ECG in normal sinus rhythm– 5 findings that suggest the patient was in an arrhythmia:
1) Abnormal QT: Either a long or short QT can cause arrhythmia, check for QTc >450 or 470-480 and assess for >half R-R interval, or <330/340(5). (Cutoffs differ depending on where you look!)
2) Brugada syndrome: Look for characteristic “coved” (big diagonal wedge-shaped) ST segments in V1-3, or “saddle back” (high and scooped) ST segments in V1-3. Brugada is not limited to but may be more common in people of Southeast Asian descent, may be unmasked with fever or some medications, and are relatively young (median age of sudden death: 41).(6)
3) ARVC (Arrhythmogenic Right Ventricular Cardiomyopathy; sometimes/previously called ARVD, for dysplasia). In my experience this is the least discussed and the hardest to describe – there’s no simple morphology that’s “usually” present. More than half have an “epsilon wave” – a small finger-like upstroke at the J point (where the QRS meets to ST segment); other signs include QRS widening or prolonged S wave in V1-3.(7)
4) HCM: look for inferior dagger Q waves (especially on the boards) and LVH.
5) WPW: I look first for a delta wave – the slurred upstroke at the start of the QRS – then for a short PR. The PR can be short for 2 reasons: first, the delta wave is taking up some of the space, so looking for a short PR can help find more subtle delta waves (and, in my experience, when I have talked to cardiologists about “is this WPW?” the first question is “Is the PR short?”). Second, the accessory pathway can insert directly onto the His-Purkinje system, so there is no slowed conduction (no delta wave) although this Lown–Ganong–Levine syndrome (LGL) might be disputed.(8)
Brief aside about PE: Pulmonary embolism is an uncommon cause of syncope and when PE does cause syncope, it is unlikely to be subtle (eg, prior VTE, tachypnea, hypotension, tachycardia, signs of DVT, or active cancer).(9-11) Brief aside about scores: Scoring systems such as the San Franscisco syncope rule have not been demonstrated to be useful enough for widespread adoption (maybe in the future some risk scores will be more helpful).(12)
Of course, “History and physical examination are the defining factors in syncope risk stratification.”(2) But, we are not as good as we think of at identifying specific causes of syncope, although very low risk patients may be easy to identify (“Consider younger patients with syncope that is nonexertional, without history or signs of cardiovascular disease, a family history of sudden death, and without comorbidities to be at low risk of adverse events.”(2)). Unfortunately, I think we are good at telling ourselves stories explaining away less straightforward syncope as vasovagal or orthostatic but are not very accurate at it.(2)
My approach is to look for concerning history and past medical history elements, and more than anything, evaluate the ECG for ischemia, blocks or the 5 concerning findings above. None of this is perfectly sensitive or specific. We cannot identify everyone at high risk without vastly over-test or over-admit, it seems reasonable to be thoughtful about who may be at higher risk for bad outcomes and thus should be hospitalized. Plus pregnancy tests for anyone who could possibly have an ectopic pregnancy.
References
2. Huff JS, Decker WW, Quinn JV, Perron AD, Napoli AM, Peeters S, Jagoda AS; American College of Emergency Physicians. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with syncope. Ann Emerg Med. 2007 Apr;49(4):431-44. doi: 10.1016/j.annemergmed.2007.02.001. PMID: 17371707.
3. https://www.ecgstampede.com/glossary/trifascicular-block/
4. https://litfl.com/trifascicular-block-ecg-library/
5. https://litfl.com/short-qt-syndrome-ecg-library/
6. https://litfl.com/brugada-syndrome-ecg-library/
7. https://litfl.com/arrhythmogenic-right-ventricular-dysplasia-arvd/
8. https://litfl.com/lown-ganong-levine-syndrome/
9. https://mdaware.blogspot.com/2016/10/pe-in-syncope-external-validation-of.html
10. https://www.nuemblog.com/blog/the-pesit-trial
11. https://www.nuemblog.com/blog/pesit
12. https://www.nuemblog.com/blog/canadian-syncope
Spine Case 10: Orthopedic Teaching: Feinberg School of Medicine
Dr. Seth Trueger, MD, MPH
Emergency Medicine, Northwestern Memorial Hospital
Associate Professor of Emergency Medicine, Feinberg School of Medicine
How To Cite This Post:
[Peer-Reviewed, Web Publication] Khawaja, Z. Hayes, D. (2026, June 26). Syncope and ECG Findings [NUEM Blog. Expert Commentary by Levine, Matthew R]. Retrieved from http://www.nuemblog.com/blog/.









Understanding odontoid process fractures and their management in the ED