

Written by: Melissa Smith, MD (NUEM ‘28) Edited by: Conner Morton, MD (NUEM ‘26)
Expert Commentary by: Megan Chenworth, MD (NUEM)
Intro:
Acute radiation injuries, while rare, can lead to significant morbidity and mortality. As these injuries have historically occurred primarily in the context of large scale disasters, emergency medicine providers should have a basic knowledge of acute radiation syndromes (ARS). Radiation injuries are classified as acute or chronic with chronic injuries generally resulting from frequent low level exposure- such as with oncologic radiation. Acute injury, however, may come from exposure during industrial accidents, to medical or food sterilization equipment, and (much less frequently) to nuclear material in reactors or via unaccounted for radionuclides. It is important to note that although large scale exposure secondary to terrorist activities has yet to occur, it remains a possibility.
Pathophysiology:
ARS may occur due to irradiation with Gamma and X rays, or via contamination by direct inoculation with radionuclides. Radiation may be expressed as units of milliseverts (mSv)- a measure of the whole body’s radiation dose-or in milligrays (mGy) -a unit of absorbed dose. Though nuanced, for the limited scope of this document these should be considered generally equivalent. In order to cause ARS, whole body radiation via a penetrating source (i.e. X rays, gamma rays, and neutrons) must occur in doses >0.7 Gy delivered over the course of minutes. For comparison, annual ambient radiation doses in the US expose a person to total body irradiation of 0.003 Gy- approximately half that of one CT scan of the chest, abdomen, or pelvis.
Disease develops as a result of both direct damage to rapidly dividing cells, and via damage to genomic data via free radical and cytokine release. Consequently, a cell’s ability to repair damage and proliferate is impaired leading to tissue atrophy, fibrosis, and death.
Stages:
ARS progresses through prodromal, latent and systemic illness phases. The prodromal phase (occurring minutes to 2 days post exposure) is generally nonspecific- presenting with nausea, vomiting, diarrhea, anorexia and lethargy as consequences of direct cellular damage. It is important to note that while patients may present with mild illness, this can quickly increase in acuity as they progress through later stages. The latent phase (within hours to 21 days post exposure) represents the asymptomatic period, during which indirect cellular damage accumulates. The systemic illness phase (hours to >60 days post exposure) is classified by the main organ system affected. Notably those with more severe presentations also demonstrate the features of the preceding less severe syndrome.
Acute Radiation Syndromes:

Figure 1: Accidental Cutaneous Radiation Injury
(CDC, 2005)
Hematopoietic Syndrome- Occurs with exposure of 1-6 Gy with a prodrome occurring at 1-6 hours and lasting 1-2 days. Affects bone marrow cells and mature lymphocytes. As such lymphopenia occurs first with associated increase in infections, worst at 2-4 weeks post exposure, and decreased antibody response. Later, around 3-4 weeks, unaffected mature cells undergoing typical cell death are not replaced secondary to bone marrow effects resulting in anemia and thrombocytopenia. Irradiated cells are also at higher oncologic risk resulting in increased incidence of hematopoietic cancers if they survive.
Gastrointestinal Syndrome- Occurs with exposure to 6-30 Gy with a prodrome occurring within 1 hour and lasting 1-2 days. For the next 4-5 days gastrointestinal mucosal cell death occurs within the latent period resulting in more severe nausea, vomiting, and diarrhea. This leads to significant metabolic losses, dehydration and hypovolemic shock. This may be complicated by sepsis as intestinal necrosis may lead to perforation which is compounded by impaired immunity associated with accompanying hematopoietic syndromes. Often fatal within 1-2 weeks.
Cerebrovascular Syndrome- Occurs at > 30 Gy and is non-survivable beyond 1-2 days. Prodrome presents within minutes and typically progresses immediately to the systemic illness phase with tremors, seizures, ataxia, and cerebral edema.
Cutaneous Radiation Injury (CRI):
CRI is a non-syndromic form of acute radiation injury and occurs with localized doses >3 Gy. It presents as a painful non-healing burn ranging in severity from erythema to necrosis often with epilation and occurs following a latent phase. Months after exposure skin may be characterized by changes in pigmentation, fibrosis, telangiectasia and fragility. CRI may occur in concurrence with ARS or alone.
Prognosis:
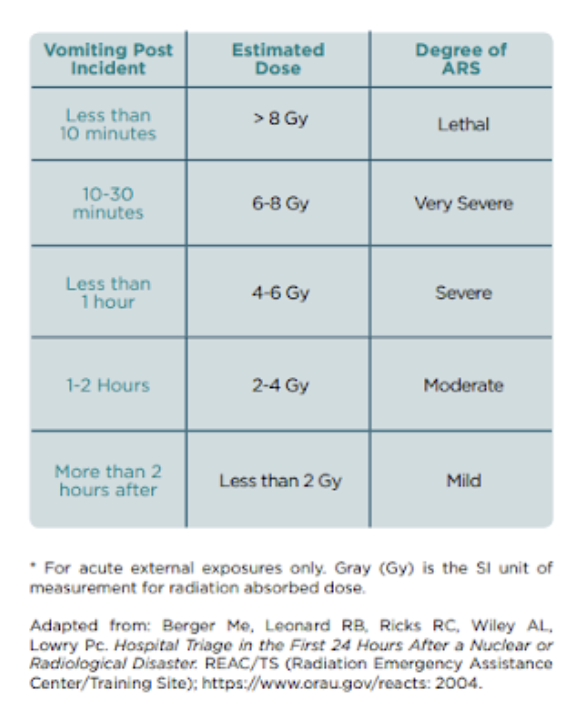
Figure 2: Estimation of External Radiation Dose Related to Onset of Vomiting
(CDC, 2023)
Prognosis is dependent on dose exposure and when a patient initially presents for care. Without medical care, exposure to 8 Gy is fatal, exposure to 3Gy has a 50% survivability, and exposure to 2Gy results in near full survivability with recovery within a month, though is associated with long term complications. With medical care exposure to 6Gy represents a 50% survival rate and some have been noted to survive up to 10 Gy exposures.
As reference: Those within 1.6 km of the 3 mile island nuclear incident were exposed to 0.00008Gy, Chernobyl evacuants to 0.03Gy and Chernobyl workers and first responders at levels up to 16Gy.
Management:
Treatment of radiologic injuries will differ based on dose and stage at presentation as well as based on singular patient exposure versus disaster settings. The concepts of traumatic injury management, decontamination, and supportive measures will, however, always apply. Care must also be taken to reduce healthcare worker exposure via reverse isolation.
In the case of unknown exposure, suspect ARS when unexplained nausea and vomiting occurs preceding pancytopenia or in the setting of non-healing unexplained wounds with epilation.
Triage and Trauma:
In the setting of a radiological disaster, triage and care of traumatic injuries, such as burns or blast wounds, takes priority as these will more imminently cause death than contamination by radioactive material. Traditional ABC’s of trauma care apply. Note that wounds visualized in this setting are not associated with CRI which occurs only after a latent phase.
Decontamination:
After addressing immediate life threats, patients should pass through decontamination. Trained staff should assist patients to remove clothing, wash out wounds first, then eye and mouth flushing if needed. Next the whole body should be gently washed with soap and water until measurement with a Geiger-Muller counter demonstrates radioactivity less than 2 times that of ambient radiation.
Patient’s may then proceed through a buffer zone and into a clean zone. If persistently high readings occur consider internal contamination via inhaled or ingested material. At this point radiation experts may suggest administration of radionuclide-specific decorporation agents which may reduce exposure by 25%-75%. Some of these specific pairings include:
-Radioactive iodine: potassium iodide
-Plutonium/yttrium/californium/americium: zinc or calcium diethylenetriamine penta-acetate
-Strontium: calcium or aluminum phosphate solutions
-Cesium/rubidium/thallium: Prussian Blue
Supportive Care and Monitoring:
-Obtain initial CBC and HLA typing prior to any necessary transfusions
-Obtain CBC’s every 2-3 hours for the first 8-12 hours and every 4-6 hours thereafter to monitor decline in lymphocytes which may help determine the dose a patient was exposed to.
-Manage fluid and electrolyte status
-Initiate broad spectrum antibiotics both IV and by mouth for protection of the GI tract
-Initiate IV antivirals and antifungals.
-Treat vomiting and pain
-Consider sedation
-If cerebrovascular syndrome is present, focus on palliation and control seizures.
-Thoroughly document onset of new symptoms as this will also assist with dose estimation and prognosis.
-Refer for necessary surgeries to be completed within 24-48 hours due to rapidly declining hematopoietic systems.
-Consult hematology early
-Report the incident to the Radiation Emergency Assistance Center/Training Site (REAC/TS) at (865) 576-3131 or (865) 576-1005
Beyond the Emergency Department:
Later management may include growth factor administration, transfusion and stem cell transplant for hematopoietic support. Skin grafts for CRI may be an option. Monitoring for cataracts and thyroid disorders will be ongoing.
Takeaways:
Although rare, acute radiological injuries can be devastating. Degree of illness and prognosis is dependent on dose exposure and a patient’s initial presentation. Emergency treatment focuses on traumatic injury management, decontamination and a focus on supportive care with close attention to prevention of infection, reverse isolation, fluid/electrolyte balances, and symptom management. Monitoring will require a team approach with radiological and hematology experts.
References:
Acosta, R., & Warrington, S. J. (2023, January 16). Radiation syndrome. StatPearls . https://www.ncbi.nlm.nih.gov/books/NBK441931/
Bushberg, J. T. (2022, December). Radiation injury . Merck Manual Consumer Version. https://www.merckmanuals.com/home/injuries-and-poisoning/radiation-injury/radiation-injury
Centers for Disease Control and Prevention. (2024, April 10). A Brochure for Physicians: Acute radiation syndrome. Centers for Disease Control and Prevention. https://www.cdc.gov/radiation-emergencies/signs-symptoms/acute-radiation-syndrome.html
Centers for Disease Control and Prevention.(2024, April 23). Acute radiation syndrome: Information for clinicians. Centers for Disease Control and Prevention. https://www.cdc.gov/radiation-emergencies/hcp/clinical-guidance/ars.html
Centers for Disease Control and Prevention. (2024, April 23). Emergency department: Evaluation and management of affected patients. Centers for Disease Control and Prevention. https://www.cdc.gov/radiation-emergencies/hcp/nuclear-detonations/evaluation-and-management.html
Centers for Disease Control and Prevention. (2023, January 13). Radiological Emergencies: Emergency Management Pocket Guide For Clinicians. U.S. Department of Health and Human Services. https://www.cdc.gov/radiation-emergencies/media/pdfs/clinicianpocketguide.pdf
Centers for Disease Control and Prevention.. (2005, June). Cutaneous radiation injury: Fact sheet for physicians. U.S. Department of Health and Human Services. https://emergency.cdc.gov/radiation/pdf/criphysicianfactsheet.pdf
Macià i Garau, M., Lucas Calduch, A., & López, E. C. (2011). Radiobiology of the acute radiation syndrome. Reports of Practical Oncology; Radiotherapy, 16(4), 123–130. https://doi.org/10.1016/j.rpor.2011.06.001
Expert Commentary

This is a great review of acute radiological injuries. It is important to remember that if there is concern for a potential radiological injury or disaster scenario, decontamination is perhaps the most important aspect of care. As mentioned, once life threats are addressed (ABCs, i.e. intubation if not protecting airway, temporary treatment of tension pneumothorax, or tourniquet of actively bleeding extremity), focus should be placed on decontamination of the patient. You can think of radioactive material as similar to sand - most of the sand comes off when you leave the beach, but the last bit needs to be physically removed to be completely rid of the exposure. Luckily, using standard precautions (decontamination and basic PPE like gowns, gloves, masks and eye protection), it is very unlikely that ED staff would receive large radiation doses from treating contaminated patients. Medical personnel working on the Chernobyl site after the accident received less than 0.1 Gy (Mettler and Voelz, NEJM, 2002; 346; 1554-1561). Lastly, any time you have concerns about a potential radiological exposure, it is important to get in touch with your entity’s Radiation Safety Officer, as they will have more information and expertise in managing these situations. Their contact information can often be found in the “Disaster Binder” that contains the emergency operation plans, including radiological exposures, located in the ED or the online copy on your site’s intranet.
Dr. Megan Chenworth
Clinical Assistant Professor, University of Pennsylvania
How To Cite This Post:
[Peer-Reviewed, Web Publication] Smith, M. Morton, C. (2026, April 11). Emergency Management of Acute Radiological Injuries [NUEM Blog. Expert Commentary by Chenworth, M]. Retrieved from http://www.nuemblog.com/blog/acute-rad-injuries.









