

Written by: Meghan Dillan, MD (NUEM ‘29) Edited by: Sasha Becker, MD (NUEM ‘27)
Expert Commentary by: Kirsten Loftus, MD, MEd (Lurie Children’s)
Expert Commentary

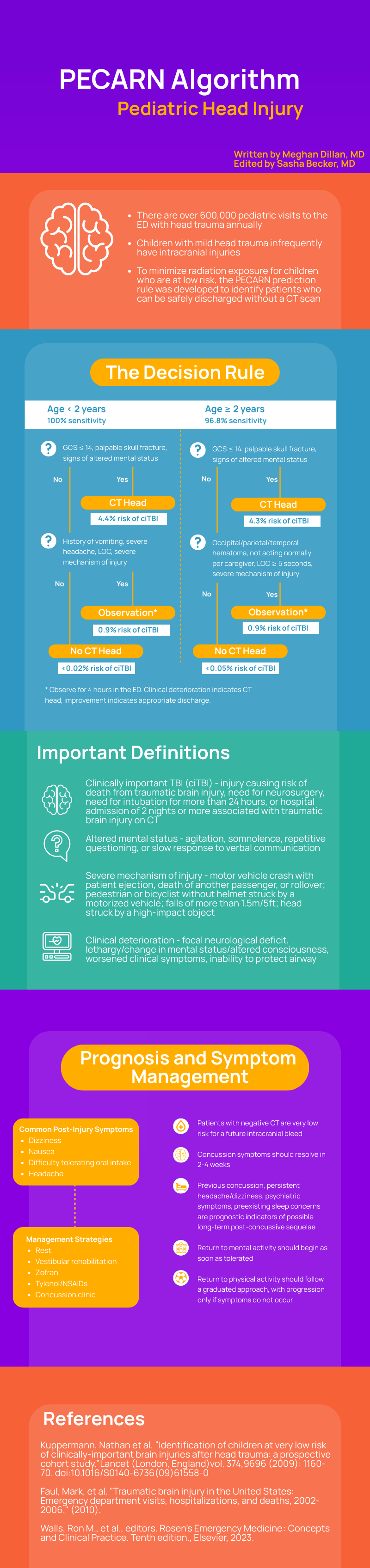
This is a high-yield summary of an approach to pediatric head injury, a clinical scenario commonly encountered across ED settings. Thankfully, there is robust pediatric-specific evidence to guide management. This post cites 3 key sources, but I would consider the Kupperman et al. prospective study to be an absolute must-read for anyone caring for children following blunt head trauma. The study aimed to identify kids who were at very low risk for clinically important TBI (ciTBI) in whom CT scan can be safely avoided and included a robust > 42,000 pediatric patients presenting across 25 EDs with blunt head trauma in their analysis. This post provides a nice visual communicating the decision rule that I use on an almost daily basis. This decision rule empowers me to 1) obtain a head CT in children with a GCS < 15, altered mental status, or a palpable skull fracture given the prevalence of ciTBI in that population, 2) safely avoid head CT in the group of children with no concerning features and therefore at very low risk for ciTBI (and importantly put families at ease with this decision based on the robust negative predictive value and additional win of avoiding unnecessary radiation on a developing brain), and 3) thoughtfully engage in shared decision-making with families surrounding observation vs head CT for the remainder that don’t fall into either of the two other groups. Some key things I’d emphasize:
- This study excluded asymptomatic kids with a trivial mechanism (e.g. walking or running into a stationary object) in order to avoid overinflating the negative predictive value and I feel similarly empowered to safely avoid a head CT in this population.
- Their goal was to identify kids at very low risk for ciTBI and not all TBIs, with ciTBI nicely defined in this post. I do discuss this with families of patients for whom I am not recommending head CT and find it well-received. I think it is also important to point out that in infants where you are concerned for child abuse, being categorized as very low risk for ciTBI should not dissuade you from proceeding with a head CT.
- Falls are among the more commonly encountered injury mechanisms, with > 5ft being considered severe in kids > 2yo and > 3ft considered severe in kids < 2yo (an easy reference for 3ft would be the height of a typical changing table).
- This study excluded patients with GCS scores < 14, where the relatively high risk of TBI on CT makes them a non-controversial group to obtain a head CT.
- For patients in the ‘observation group’ with an overall low risk of ciTBI, this as an observation vs head CT group and I enjoy engaging in shared decision-making with families. Based on this paper, I strongly consider head CT if there are multiple findings (e.g. LOC and severe mechanism), but favor observation for an isolated finding (e.g. history of vomiting without other findings), with the latter practice further supported by multiple secondary analyses of this study finding very low prevalences of ciTBI in children with isolated findings including isolated vomiting, severe mechanism, and LOC.[1][2][3]
I appreciate that this post additionally walks through prognosis and management considerations. Focus often centers on the decision-making around head CT, but it is equally important for patients being discharged home to set expectations around the clinical course, supportive care, and return to activities. I routinely encourage close follow-up with the child’s pediatrician so that families have a touch point to reassess their child’s symptoms and help support return to activities.
Dr. Kirsten Loftus, MD, MEd
Division of Pediatric Emergency Medicine, Lurie Children’s Hospital of Chicago
Assistant Professor of Pediatrics, Feinberg School of Medicine
Commentary References:
[1] Dayan PS, Holmes JF, Atabaki S, Hoyle J Jr, Tunik MG, Lichenstein R, Alpern E, Miskin M, Kuppermann N; Traumatic Brain Injury Study Group of the Pediatric Emergency Care Applied Research Network (PECARN). Association of traumatic brain injuries with vomiting in children with blunt head trauma. Ann Emerg Med. 2014 Jun;63(6):657-65. doi: 10.1016/j.annemergmed.2014.01.009. Epub 2014 Feb 19. PMID: 24559605.
[2] Nigrovic LE, Lee LK, Hoyle J, Stanley RM, Gorelick MH, Miskin M, Atabaki SM, Dayan PS, Holmes JF, Kuppermann N; Traumatic Brain Injury (TBI) Working Group of Pediatric Emergency Care Applied Research Network (PECARN). Prevalence of clinically important traumatic brain injuries in children with minor blunt head trauma and isolated severe injury mechanisms. Arch Pediatr Adolesc Med. 2012 Apr;166(4):356-61. doi: 10.1001/archpediatrics.2011.1156. Epub 2011 Dec 5. Erratum in: Arch Pediatr Adolesc Med. 2014 Jun;168(6):586. PMID: 22147762.
[3] Lee LK, Monroe D, Bachman MC, Glass TF, Mahajan PV, Cooper A, Stanley RM, Miskin M, Dayan PS, Holmes JF, Kuppermann N; Traumatic Brain Injury (TBI) Working Group of Pediatric Emergency Care Applied Research Network (PECARN). Isolated loss of consciousness in children with minor blunt head trauma. JAMA Pediatr. 2014 Sep;168(9):837-43. doi: 10.1001/jamapediatrics.2014.361. PMID: 25003654.
How To Cite This Post:
[Peer-Reviewed, Web Publication] Dillan, M. Becker, S. (2026, April 26). PECARN: Pediatric Head Injury [NUEM Blog. Expert Commentary by Loftus, K]. Retrieved from http://www.nuemblog.com/blog/pecarn.









