Written by: Kendra Jeans MD (NUEM ‘28) Edited by: Dean Hayes, MD (NUEM ‘27)
Expert Commentary by: Nathan Trueger, MD (NUEM)
Expert Commentary

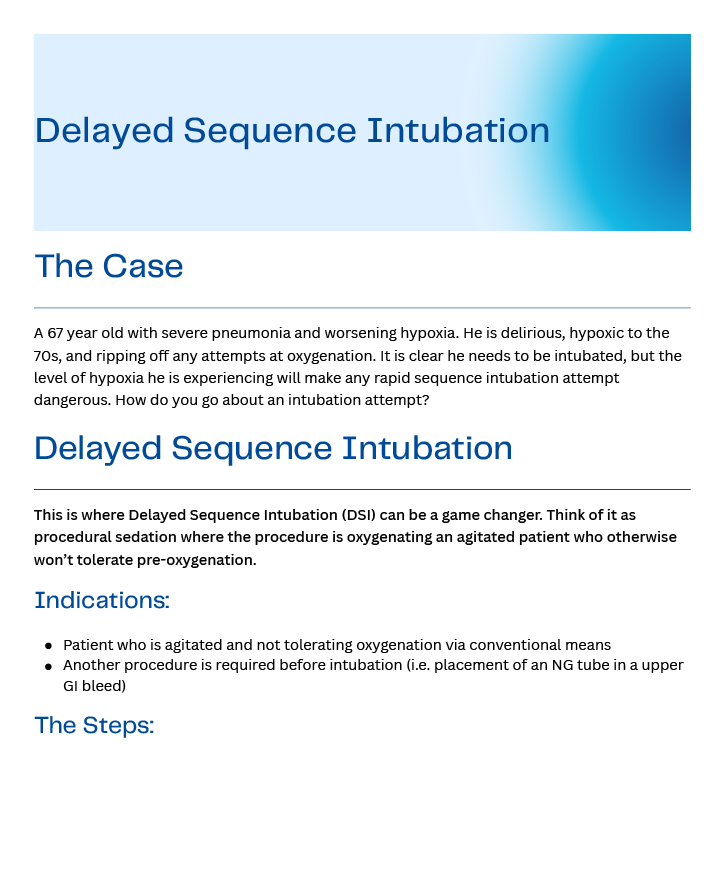
Thank you Dr. Jeans and Dr. Hayes for this excellent overview of DSI. The Case at the top is the perfect illustration of DSI’s place:
For most patients requiring intubation, paralytics (aka, neuromuscular blocking agents, NMBA) optimize the glottic view and first pass success. We also give sedatives so the experience is not horrible for patients.
For most ED patients requiring intubation, RSI is safest because the (near) simultaneous administration of sedative and NMBA – with appropriate preoxygenation – allows us to avoid positive pressure (ie, bagging) which increases the risk of gastric insufflation and therefore vomiting, risking aspiration and making intubation more difficult. The key here is that patients need sufficient preoxygenation to survive the apneic period.[1]
(Aside #1: this is what patients with predicted difficult aware anatomy may be more appropriate for “awake” intubation, ie, topical lido + sedation.[2] See also the last paragraph below.)
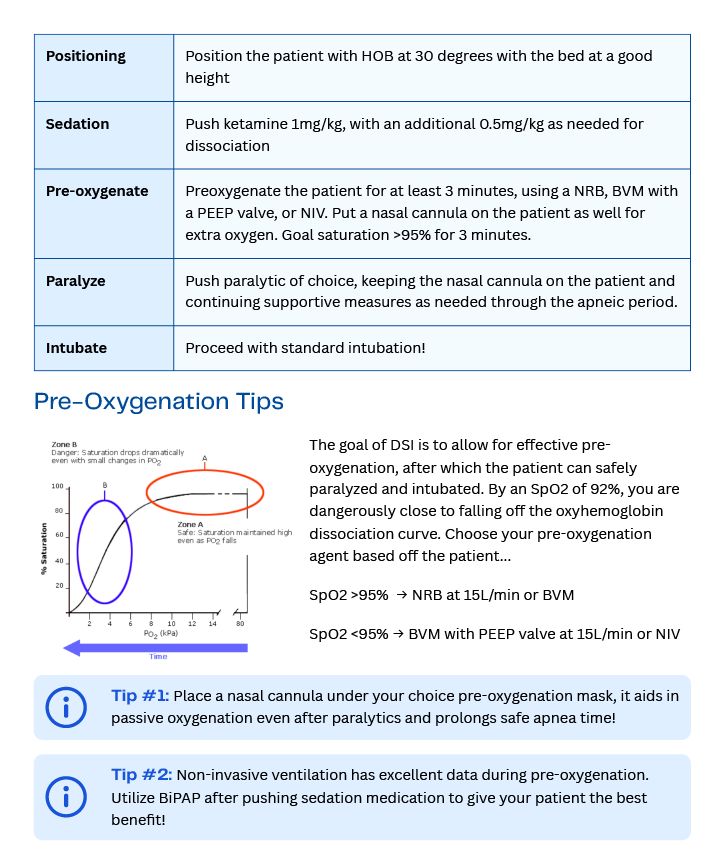
However, some patients may be too delirious to allow proper preoxygenation. In this case, the idea is essentially procedural sedation for the procedure for preoxygenation. Most patients will then be able to safely preoxygenate on their own, either with standard nasal cannula/reservoir facemask, or, if they require PEEP or more support, NIPPV (which is probably safer than bagging, as discussed above, which can be done if needed). Then, NMBA, and proceed as usual.
(Aside 2: I think of the general rule to avoid NIPPV in altered patients so as to avoid aspiration absolutely appropriate in general, eg, for patients sitting alone in a room in the ER or a general hospital floor for hours; in cases like ours, we are talking about critically ill patients where we are continuously at their side entirely prepared to intubate, using NIPPV for a matter of minutes under close monitoring.)
Ketamine is probably the best choice here as it has the least likelihood of impairing respiratory drive and protective airway reflexes.[1] Otherwise, much like the preoxygenation, pretty much every element is whatever is appropriate, eg direct or video or hyperangulated laryngoscopy, succinylcholine or rocuronium, stylet or bougie, and so on.
The alternative / “old way” was to push RSI meds and hope we can bag them up before they desaturate, which strikes me as much riskier. For what it’s worth, 0 of the 62 patients in the original DSI study aspirated.[3]
Lastly, I will point out that a lot of the great work by Scott Weingart of EMCrit can be somewhat confusing as there is a lot of overlap with things like ketamine and NIPPV and I find mentally separating the elements of airway management is helpful in keeping it all straight.[4]
References
1) Walls R, Murphy M. Manual of Emergency Airway Management. 2008. 3rd Edition, Lippincott Williams & Wilkins, Philadelphia.
2) https://mdaware.blogspot.com/2014/01/awake-intubation-screencast.html
3] Weingart SD, Trueger NS, Wong N, Scofi J, Singh N, Rudolph SS. Delayed sequence intubation: a prospective observational study. Ann Emerg Med. 2015 Apr;65(4):349-55. doi: 10.1016/j.annemergmed.2014.09.025. Epub 2014 Oct 23. PMID: 25447559.
3) https://mdaware.blogspot.com/2012/06/ketamine-is-heckuva-drug.html
Dr. Nathan Trueger, MD
Emergency Medicine, Northwestern Memorial Hospital
Associate Professor of Emergency Medicine, Feinberg School of Medicine
How To Cite This Post:
[Peer-Reviewed, Web Publication] Jeans, K. Hayes, Dean. (2026, July 15). Delayed Sequence Intubation [NUEM Blog. Expert Commentary by Trueger, Nathan]. Retrieved from http://www.nuemblog.com/blog/delayed-sequence-intubation.