

Written by: Meghan Dillan, MD (NUEM ‘29) Edited by: Alexander Reardon, MD (NUEM ‘26)
Expert Commentary by: Matthew R. Levine, MD (NUEM)
Expert Commentary

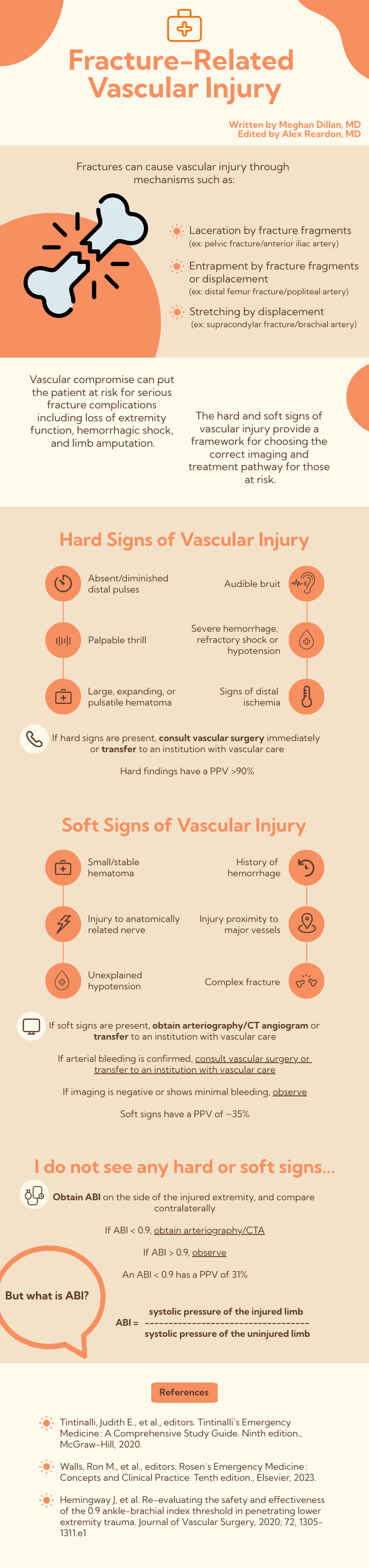
Vascular injury from sharp fracture fragments are indeed time-sensitive limb threats and must proceed with aggressive management as described by Dr Dillan.
However, many pulse deficits after fractures, as mentioned, are from traction or stretching, not from vascular transection. These injuries are treated with timely reduction, not initial vessel imaging. A classic example would be a bi- or tri- malleolar ankle fracture with joint subluxation. These patients often arrive with visible deformity and pedal pulse deficit. These should be rapidly reduced (with or without x rays) and then the vascular exam is repeated. If the repeat exam is normal, typically no further vascular imaging is required. Delaying reduction in these cases for vascular imaging would not only prolong ischemic time and traction on the affected vessel, but would not necessarily subsequently be indicated.
However, if the vascular injury is thought to be from a sharp fracture fragment, then of course emergently consult specialists or transfer to where the resources are available. Do not let imaging tests delay emergent consultation or transfer.
Nuance and experience play an important role in applying “soft criteria”. Not all soft criteria are created equal. A neuro deficit after a penetrating mechanism is highly concerning for vascular injury since nerves and arteries are often so closely anatomically associated. Image those! However, the soft criteria of small hematoma, proximity to vascular structure, and complex fracture are all vague, open to varying interpretations, and certainly don’t always lead to or require vessel imaging. While keeping the possibility of vascular injury in your ddx, this is where gestalt, pattern recognition, and the “art of medicine” will lead to proper cost-effective resource utilization and safe patient management.
Dr. Matthew R. Levine, MD
Emergency Medicine, Northwestern Memorial Hospital
Associate Professor of Emergency Medicine, Feinberg School of Medicine
How To Cite This Post:
[Peer-Reviewed, Web Publication] Dillan, M. Reardon, A. (2026, April 30). Fracture-Related Vascular Injury [NUEM Blog. Expert Commentary by Levine, Matthew R]. Retrieved from http://www.nuemblog.com/blog/fracture-vascular-injury.









