

Recognize the signs of bupropion toxicity and grow competent with its management.
Posts tagged #psychiatry
COVID-19 and Mental Health

Written by: Evelyn Huang, MD (NUEM ‘24) Edited by: Julian Richardson (NUEM ‘21)
Expert Commentary by: Tyler Black, MD, FRCPC
COVID-19 has been difficult for everyone. Deaths, isolation, loss of work, and countless other hardships abound. With this, comes the concern for mental health crises. In a survey from June 2020, 11% of adults reported thoughts of suicide in the past 30 days [1]. It can be hypothesized that the pandemic has increased suicide rates. However, does this bear out in the literature? As frontline workers, and oftentimes the only interaction that patients have with the healthcare system, it is particularly important that we identify the impact of COVID-19 on the mental health of the patients that we see every day.
In Japan, researcher used a cross-sectional study to analyze national suicide rates during the COVID-19 pandemic. They found that suicide rates in 2020 were increased in October and November for men and in July through November for women when compared to 2016-2019. Increases in suicide rates were more pronounced with men and women that are younger than 30 [2]. This supports the idea that suicide rates increased as a result of the pandemic, especially with the younger population.
However, the trends in the United States are different. A study conducted in the US looked at suicide rates in Massachusetts from March to May 2020. Excluding data from pending death investigations, they found that the incident rate for suicide death was 0.67 per 100,000 person-months for the pandemic period as compared to 0.80 in the corresponding period in 2019. The researchers point to a sense of shared purpose, connections via video platforms, anticipated government aid, and mental health awareness campaigns as possible explanations for the stable rate of suicide deaths [3]. Another study looked at United States suicide related searches during the beginning of the pandemic. Researchers found that internet searches for suicide decreased during the early stages of the COVID pandemic (March to July 2020). While this may be surprising, there is literature that shows that catastrophic events can be associated with increased social support and reduce suicidal outcomes [4]. However, as the pandemic lengthens, more research is needed to see the trends in the data.
The next question is whether the same trend of decreased suicidality also applies to the pediatric population. A pediatric emergency department in Texas looked at the resulted of their routine suicide risk screenings for patients aged 11-21. They found a significantly higher rate of suicidal ideation in March and July 2020 and a higher rate of suicide attempts in February, March, April, and July 2020 when compared to the same months in 2019 [5]. It has also been cited that prior to the pandemic, suicide was the 10th leading cause of death in the United States, but the 2nd leading cause of death among people aged 12-17 [1]. This makes our interactions with the pediatric population even more important and argues for suicide risk screening for every patient.
Looking historically, there are differing trends for different global catastrophes. One researcher found that World War I did not influence United States suicide rates, whereas the great Influenza Epidemic increased suicide rates [6]. Another study looked at suicide rates in Hong Kong during the Severe Acute Respiratory Syndrome (SARS) outbreak in 2003. They found an increase in older adult suicide in April 2003 when compared to 2002. These researchers cited loneliness and disconnectedness in the older community as a possible explanation [7]. While there are many different factors that go into increased suicidality, trends seen in the past can help guide policy and actions today.
Research is still needed to look at the current trends of suicide rates. The question is whether suicide rates will change as the pandemic continues to lengthen and the sense of shared purpose wanes and social isolation continues. The mental health of our patients is likely to be impacted long after the pandemic ends.
A study conducted in California found that emergency department patients presenting with deliberate self-harm or suicidal ideation had an increased risk of suicide or other mortality during the first year after their initial presentation in the emergency department [8]. This is a troubling trend, but also presents an opportunity for improvement. As emergency physicians, it is also important that we keep vigilant and take the time to talk about mental health. A common fear is that asking about suicide will prompt suicidal ideation, but research has shown that this is not the case [9]. There are several suicide screening tools that can be used in the ED, such as the Suicide Assessment 5‐step Evaluation and Triage (SAFE‐T) and American College of Emergency Physicians ICAR2E [9]. What is important is to ask, because patients will often reveal things to us that they do not mention to their loved ones. Build suicide screenings into your general practice, watch out for risk factors, and support those that are seek help.
References
1. Panchal, Nirmita, et al. The Implications of COVID-19 for Mental Health and Substance Use. Kaiser Family Foundation, 10 Feb. 2021, www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use/.
2. Sakamoto H, Ishikane M, Ghaznavi C, Ueda P. Assessment of Suicide in Japan During the COVID-19 Pandemic vs Previous Years. JAMA Netw Open. 2021;4(2):e2037378. doi:10.1001/jamanetworkopen.2020.37378
3. Faust JS, Shah SB, Du C, Li S, Lin Z, Krumholz HM. Suicide Deaths During the COVID-19 Stay-at-Home Advisory in Massachusetts, March to May 2020. JAMA Netw Open. 2021;4(1):e2034273. doi:10.1001/jamanetworkopen.2020.34273
4. Ayers JW, Poliak A, Johnson DC, et al. Suicide-Related Internet Searches During the Early Stages of the COVID-19 Pandemic in the US. JAMA Netw Open. 2021;4(1):e2034261. doi:10.1001/jamanetworkopen.2020.34261
5. Hill RM, Rufino K, Kurian S, Saxena J, Saxena K, Williams L. Suicide ideation and attempts in a pediatric emergency department before and during COVID-19. Pediatrics. 2020; doi: 10.1542/peds.2020-029280
6. Wasserman IM. The impact of epidemic, war, prohibition and media on suicide: United States, 1910-1920. Suicide Life Threat Behav. 1992 Summer;22(2):240-54. PMID: 1626335.
7. Cheung YT, Chau PH, Yip PS. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int J Geriatr Psychiatry. 2008 Dec;23(12):1231-8. doi: 10.1002/gps.2056. PMID: 18500689.
8. Goldman-Mellor S, Olfson M, Lidon-Moyano C, Schoenbaum M. Association of Suicide and Other Mortality With Emergency Department Presentation. JAMA Netw Open. 2019;2(12):e1917571. doi:10.1001/jamanetworkopen.2019.17571
9. Brenner, J. M., Marco, C. A., Kluesner, N. H., Schears, R. M., & Martin, D. R. (2020). Assessing psychiatric safety in suicidal emergency department patients. Journal of the American College of Emergency Physicians Open, 1(1), 30-37.
Expert Commentary
This review is a comprehensive summary of the challenges and nuances of suicide epidemiology. Though it goes against the narrative many hold, in the United States we have preliminary but reliable data for suicides two years into the pandemic, we have not seen an increase in suicide rate in any age group (Figure 1) [1,2]. This reassuring news is tempered by the knowledge that prior to the pandemic, a decade-long trend of increasing suicide rates has maintained, and children, adults, and older adults are much more likely to die of suicide now in America than they were in 2010 [3].

Figure 1. Odds ratio for suicide, by age groups (A = under 18 years; B = 18 to 64 years; C = above 64 years). Years are grouped to match with the onset of the pandemic (March 2020), such that each data point represents April of that year to the following March (instead of the typical January to December presentation). The comparator for each year’s odds of suicide is a sum of the odds between April 2017 and March 2020. The shaded vertical lines represent the 95% confidence interval for odds ratio, and they are hidden behind the markers for the adult group due to the small confidence interval.
Whenever considering suicide risk, it is crucial to remember that there are not direct links between suicidal thinking, suicide attempts or visits to the emergency department, and deaths by suicide. Up to 60% of people die of suicide on their first attempt, and the vast majority (95%) of people who attempt suicide do not die of suicide, so while it is important to see the danger in suicidal presentations to emergency department, it is crucial to be aware of the challenges in predicting who will live and who will die by suicide and focus on a person-centered approach to understanding an individual’s risk and protective factors[4, 5].
I applaud the authors for encouraging all clinicians to consider suicide risk in all patients and to become comfortable with routine screening. This may never demonstrate a reduction in suicide rates in rigorous research, but we have ample evidence that having open, genuine discussions about psychological, social, and health problems regarding suicide risk is beneficial to the patients we care for [6].
References
1. Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Mortality 1999-2020 on CDC WONDER Online Database, released in 2021. Data are from the Multiple Cause of Death Files, 1999-2020, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. Accessed at http://wonder.cdc.gov/ucd-icd10.html on Dec 1, 2022.
2. Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Provisional Mortality on CDC WONDER Online Database. Data are from the final Multiple Cause of Death Files, 2018-2020, and from provisional data for years 2021-2022, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. Accessed at http://wonder.cdc.gov/mcd-icd10-provisional.html on Dec 1, 2022
3. Centers for Disease Control and Prevention. (2022, June 28). Suicide data and statistics. Centers for Disease Control and Prevention. Retrieved December 1, 2022, from https://www.cdc.gov/suicide/suicide-data-statistics.html
4. Bostwick, J. M., Pabbati, C., Geske, J. R., & McKean, A. J. (2016). Suicide attempt as a risk factor for completed suicide: Even more lethal than we knew. American Journal of Psychiatry, 173(11), 1094–1100.
5. Hawton, K., Lascelles, K., Pitman, A., Gilbert, S., & Silverman, M. (2022). Assessment of suicide risk in mental health practice: shifting from prediction to therapeutic assessment, formulation, and risk management. The Lancet Psychiatry.
6. Dazzi, T., Gribble, R., Wessely, S., & Fear, N. T. (2014). Does asking about suicide and related behaviours induce suicidal ideation? What is the evidence?. Psychological medicine, 44(16), 3361-3363.

Tyler Black, MD, FRCPC
Assistant Clinical Professor
Department of Psychiatry
The University of British Columbia
How To Cite This Post:
[Peer-Reviewed, Web Publication] Huang, E. Richardson, J. (2023, Jan 2). COVID-19 and Mental Health. [NUEM Blog. Expert Commentary by Black, T]. Retrieved from http://www.nuemblog.com/blog/covid-mental-health
Other Posts You May Enjoy









Droperidol

Written by: Adam Payne, MD (NUEM ‘24) Edited by: Julian Richardson, MD (NUEM ‘21) Expert Commentary by: Matt O' Connor, MD

Expert Commentary
Thanks to Dr. Payne & Dr. Richardson for putting this together! I think this was well done, they’ve presented a concise overview of the safety and efficacy of droperidol.
There’s a lot of utility in droperidol. It’s great for nausea, migraines, and even as an adjunct for chronic pain. It’s also a very good choice for agitation. I use it most often for nausea. It’s been shown to be as effective as odansetron, and more effective than metoclopramide. Anecdotally, I find it works particularly well for gastroparesis and cannabinoid hyperemesis (with some low-concentration topical capsaicin cream), with less sedation than haloperidol. For migraines, it has been shown to be as effective as prochlorperazine. It works well for sedation in agitated patients as well; IV & IM it has a much faster onset than haloperidol, and so benzodiazepines typically do not have to be co-administered, reducing the level and duration of sedation and need for monitoring.
The black box warning significantly limited droperidol’s availability, such that many of our newer graduates have not had any first-hand clinical experience with the medication. If you’re not familiar with its use, don’t let the black box warning completely dissuade you. Subsequent studies looking at emergency department droperidol use have shown it to be safe, and that complications related to QT prolongation are rare in typical doses. As a rule of thumb, the dose of droperidol is about half of the dose of haloperidol for a given indication. For nausea, migraine, or other pain, I usually start with 0.625-2.5mg IV, twice that IM, and can repeat dosing if needed (my most common starting dose is 1.25mg IV). For agitation, usually 2.5-5mg IM, though up to 10mg IM has been shown likely to be safe. Although it is prudent to be cautious, I think the literature supports droperidol’s use at appropriate doses in otherwise healthy patients.

Matt O’Connor, MD
Emergency Medicine Physician
BerbeeWalsh Department of Emergency Medicine
University of Wisconsin Hospitals and Clinics
How To Cite This Post:
[Peer-Reviewed, Web Publication] Payne, A. Richardson, J. (2021, Aug 30). Droperidol. [NUEM Blog. Expert Commentary by O’Connor, M]. Retrieved from http://www.nuemblog.com/blog/droperidol
Other Posts You May Enjoy









Hanging Injuries

Written by: Vytas Karalius, MD, MPH (NUEM ‘22) Edited by: Nery Porras, MD (NUEM ‘21) Expert Commentary by: Kevin Emmerich, MD, MS
Today’s post was inspired by the near-hanging of young gentleman who ended up passing away due to complications related to his near-hanging. His parents decided to donate his organs to Gift of Hope, allowing the passing of his life to extend the lives of others. While we hope to never see cases like these, they are an inevitable part of our job as emergency medicine physicians. As with most rare and complex pathology, preparation and knowledge can help us with the management of these cases when things often get chaotic. Lastly, as emergency medicine physicians who see the sequelae of mental illness daily in their EDs, I encourage us all to advocate for better funding and access to mental health care in the United States.
Hanging Injury
Terms/Classification [1]
“Hanging” is used to describe a death from a form of strangulation that involves hanging from the neck.
“Near-hanging” is a term for patients who have survived an attempted hanging (or at least long enough to reach the hospital).
“Complete hanging” defines when a patient’s legs are fully suspended off the ground and the patient's bodyweight is fully suspended by the neck.
“Incomplete hanging” defines when some part of the patient’s body is still on the ground and the body's full weight is not suspended off the ground.
“Judicial hanging” classically refers to victims who fell at least the height of their body.
Epidemiology:
Hanging is the 2nd most common form of successful suicide in the US after firearms
Accounts for 23% of >34,500 suicides in 2007
In the jail system, hanging is the most common form of successful suicide
Increasing incidence in US
Risk Factors: male, aged 15-44 years, history of drug or alcohol abuse, history of psychiatric illness
Pathophysiology of Injury:
Spine/Spinal Cord:
When the drop is greater than or equal to the height of the victim, as in a judicial hanging, there will almost always be cervical spine injury.
The head hyperextends, leading to fracture of the upper cervical spine ("hangman's fracture” of C2) and transection of the spinal cord.
Cervical injuries are in non-judicial hangings are rare. [2] One retrospective case review of near-hangings over a 10-year period found the incidence of cervical spine fracture to be as low as 5%. [3]
Vascular:
The major pathologic mechanism of death in hanging/strangulation is neck vessel occlusion, not airway obstruction. [1,4]
Death ultimately results from cerebral hypoxia and global ischemia.
There are two mechanisms by which this happens:
Venous: The most implicated cause of death is actually venous obstruction. Jugular veins are superficial and easily compressible. Obstruction of venous outflow from the brain leads to stagnant hypoxia and loss of consciousness in as little as 15 seconds.
Arterial: The risk of damage to the major arterial blood flow to the brain (such as carotid artery dissection) is rare, but should suspected in patients. [4]
Cardiac:
Carotid body reflex-mediated cardiac dysrhythmias are reported, and likely a minor mechanism of death.
Pulmonary:
Airway compromise plays less of a role in the immediate death of complete hanging/strangulation. However, it is a major cause of delayed mortality in near-hanging victims. [1,4]
Significant pulmonary edema occurs through two mechanisms:
Neurogenic: centrally mediated, massive sympathetic discharge; often in association with serious brain injury and a poor prognostic implication.
Post-obstructive: strangulation causes marked negative intrapleural pressure, generated by forceful inspiratory effort against extra-thoracic obstruction; when the obstruction is removed, there is a rapid onset pulmonary edema leading to ARDS.
Aspiration pneumonia later sequela of near-hanging injury.
Airway edema from mechanical trauma to the airway, which can make intubation difficult.
Tracheal stenosis can develop later in the hospital course.
Other Injuries:
Hyoid bone fracture
Cricoid or thyroid cartilage injury [5]
Physical Examination:
"Ligature marks" or abrasions, lacerations, contusions, bruising, edema of the neck
Tardieu spots of the eyes
Severe pain on gentle palpation of the larynx (laryngeal fracture)
Respiratory signs: cough, stridor, dysphonia/muffled voice, aphonia
Varying levels of respiratory distress
Hypoxia
Mental status changes
Early Management/Stabilization:
ABCs as always
Early endotracheal intubation may become necessary with little warning.
Patients who are unconscious or have symptoms such as odynophagia, hoarseness, neurologic changes, or dyspnea require aggressive airway management.
If ETI unsuccessful, consider cricothyroidotomy; if unsuccessful, percutaneous trans-laryngeal ventilation may be used temporarily.
Judicious and cautious fluid resuscitation - avoid large fluid volume resuscitation and consider early pressors, as fluids increases the risk/severity of ARDS and cerebral edema.
Monitor for cardiac arrhythmias.
The altered/comatose patient should be assumed to have cerebral edema with elevated ICP.
Imaging/Further Testing:
Chest radiograph
CT brain
CT C-spine
CTA head/neck
Can consider soft-tissue neck x-ray, if CT not immediately available
Further Management:
In patients with signs of hanging/strangulation, there should be a low threshold to obtain diagnostic imaging/testing as discussed above.
Expect pulmonary complications early.
They are a major cause of delayed mortality in near-hanging victims, as stated above.
Early intubation and airway management are important.
Non-intubated patients with pulmonary edema may benefit from positive end-expiratory pressure ventilation.
Patients with symptoms of laryngeal or tracheal injury (e.g. dyspnea, dysphonia, aphonia, or odynophagia), should undergo laryngobronchoscopy with ENT. [4,6]
Tracheal stenosis has been reported during the hospital course. Address cerebral edema from anoxic brain injury, using strategies to reduce intracranial pressure or seizure prophylaxis. [4]
Address vascular complications seen on CTA and coordinate intervention with the appropriate specialty at your institution.
Therapeutic Hypothermia
There is some evidence for therapeutic hypothermia in those with cardiac arrest from hanging injury [7,8] and those who are comatose from hanging injury. [9-11] While the evidence is weak, in the absence of better evidence, it is reasonable to consider hypothermia treatment in all comatose near-hanging victims. [1,12,13]
When suicide is suspected, evaluate patients for other methods of self-harm (e.g. wrist lacerations, self-stabbing, ingestions). It is also important to consider drug and alcohol intoxication. [4]
Disposition:
Admit critically ill patients to the appropriate ICU-level care.
Admit patients with abnormal radiologic or endoscopic imaging to the appropriate service and level of care.
Even if the initial presentation is clinically benign, all near-hanging victims should be observed for 24 hours, given the high risk of delayed neurologic, airway and pulmonary complications. [14]
Observe asymptomatic patients with normal imaging.
Psychiatry/Crisis Team consult on all suspected intentional cases.
Emphasize strict return precautions as well as education about possible delayed respiratory and neurologic dysfunction when discharging patients.
Some patients may require transfer to a trauma center if the required services are not available at the initial receiving facility. [1]
Prognostication:
GCS 3/GCS 3T is a predictor of very poor outcome, [15-19] but there is mixed evidence on the GCS as a predictor of outcomes in GCS scores greater than 3, especially with regard to neurologic intactness. [3,19]
Recovery of patients with neurology symptoms is unpredictable. [4]
Patients presenting with cardiac arrest have a very poor prognosis, and might be the strongest predictor of poor prognosis. [4,8,16,18,20]
Other predictors of poor clinical outcome include:
Anoxic brain injury or cerebral edema on head CT [3,19]
Prolonged hanging time [18]
Cardiopulmonary arrest [8,11,19]
Cervical spine injury
Hypotension on arrival
Expert Commentary
We’ve all certainly been involved with a patient with reported hanging injury at some point in our time in the ED. They are usually unimpressive if a person does it as more of a gesture rather than a true suicide attempt. When they are unfortunately done “correctly,” they usually result in a trip to the morgue instead of the ED. When the swiss cheese holes align and a true hanging attempt results in a serious but not fatal presentation, things can get quite hairy. I’ve been a part of one such case, and will never forget it. Here are my two cents.
Airway
This should undoubtedly be treated as a predicted difficult airway, not only due to likely cervical spine trauma, but also possibly due to airway edema. Get your ducks in a row for this unless this patient is crashing in front of you. Get your consultants/help (if available), preoxygenate, airway adjuncts open and ready, backup airway supplies if your first plan fails. Most importantly, have a plan and discuss this with your team beforehand. Don’t be afraid to take an awake look with a hyperangulated video laryngoscope, especially if this patient presents with stridor. Ketamine can be your friend here. This should be an airway that you do not undertake without a scalpel, finger, and bougie ready just in case. I like to draw a line on the patient’s skin overlying the cricothyroid membrane beforehand.
Trauma
Self explanatory, but don’t be stingy here. Light this patient up from head to pelvis, including the neck angiogram. Document a repeat neuro exam every time you move this patient.
Overdose/psych
Don’t forget your Tylenol and salicylate levels, EKG in this suicide attempt. If you feel the need to add the useless urine drug screen, I suppose this is fine as well.

Kevin Emmerich, MD, MS
Emergency Medicine Physician
Methodist Hospital
Gary, Indiana
How To Cite This Post:
[Peer-Reviewed, Web Publication] Karalius, V. Porras, N. (2021, Aug 9). Hanging Injuries. [NUEM Blog. Expert Commentary by Emmerich, K]. Retrieved from http://www.nuemblog.com/blog/hanging-emergencies
Other Posts You May Enjoy








References
1. Walls RM, Hockberger RS, Gausche-Hill M. Rosen's emergency medicine : concepts and clinical practice. Ninth edition. ed. Philadelphia, PA: Elsevier; 2018.
2. Aufderheide TP, Aprahamian C, Mateer JR, et al. Emergency airway management in hanging victims. Ann Emerg Med. 1994;24(5):879-884.
3. Salim A, Martin M, Sangthong B, Brown C, Rhee P, Demetriades D. Near-hanging injuries: a 10-year experience. Injury. 2006;37(5):435-439.
4. Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM. Tintinalli's emergency medicine: a comprehensive study guide. 9th. ed. New York: McGraw-Hill Education; 2019.
5. Tugaleva E, Gorassini DR, Shkrum MJ. Retrospective Analysis of Hanging Deaths in Ontario. J Forensic Sci. 2016;61(6):1498-1507.
6. Hackett AM, Kitsko DJ. Evaluation and management of pediatric near-hanging injury. Int J Pediatr Otorhinolaryngol. 2013;77(11):1899-1901.
7. Hsu CH, Haac B, McQuillan KA, Tisherman SA, Scalea TM, Stein DM. Outcome of suicidal hanging patients and the role of targeted temperature management in hanging-induced cardiac arrest. J Trauma Acute Care Surg. 2017;82(2):387-391.
8. Kim MJ, Yoon YS, Park JM, et al. Neurologic outcome of comatose survivors after hanging: a retrospective multicenter study. Am J Emerg Med. 2016;34(8):1467-1472.
9. Jehle D, Meyer M, Gemme S. Beneficial response to mild therapeutic hypothermia for comatose survivors of near-hanging. Am J Emerg Med. 2010;28(3):390.e391-393.
10. Lee BK, Jeung KW, Lee HY, Lim JH. Outcomes of therapeutic hypothermia in unconscious patients after near-hanging. Emerg Med J. 2012;29(9):748-752.
11. Hsu CH, Haac BE, Drake M, et al. EAST Multicenter Trial on targeted temperature management for hanging-induced cardiac arrest. J Trauma Acute Care Surg. 2018;85(1):37-47.
12. Borgquist O, Friberg H. Therapeutic hypothermia for comatose survivors after near-hanging-a retrospective analysis. Resuscitation. 2009;80(2):210-212.
13. Sadaka F, Wood MP, Cox M. Therapeutic hypothermia for a comatose survivor of near-hanging. Am J Emerg Med. 2012;30(1):251.e251-252.
14. McHugh TP, Stout M. Near-hanging injury. Ann Emerg Med. 1983;12(12):774-776.
15. Kao CL, Hsu IL. Predictors of functional outcome after hanging injury. Chin J Traumatol. 2018;21(2):84-87.
16. La Count S, Lovett ME, Zhao S, et al. Factors Associated With Poor Outcome in Pediatric Near-Hanging Injuries. J Emerg Med. 2019;57(1):21-28.
17. Martin MJ, Weng J, Demetriades D, Salim A. Patterns of injury and functional outcome after hanging: analysis of the National Trauma Data Bank. Am J Surg. 2005;190(6):836-840.
18. Matsuyama T, Okuchi K, Seki T, Murao Y. Prognostic factors in hanging injuries. Am J Emerg Med. 2004;22(3):207-210.
19. Nichols SD, McCarthy MC, Ekeh AP, Woods RJ, Walusimbi MS, Saxe JM. Outcome of cervical near-hanging injuries. J Trauma. 2009;66(1):174-178.
20. Gantois G, Parmentier-Decrucq E, Duburcq T, Favory R, Mathieu D, Poissy J. Prognosis at 6 and 12months after self-attempted hanging. Am J Emerg Med. 2017;35(11):1672-1676.
Malingering in the Emergency Department
Written by: Aaron Wibberley, MD (PGY-2) Edited by: Kaitlin Ray, MD (PGY-4) Expert commentary by: Chris Lipp, MD

Expert Commentary
Malingering is a patient behaviour with a profound hazard: the misdiagnosis of a “deceptive” patient who in reality has a serious medical illness. Chief complaints associated with malingering may coincide with a vast differential of possibilities: neck pain, symptoms after head trauma, and abdominal pain. Just like musculoskeletal back pain is a diagnosis of exclusion for a patient presenting with acute discomfort, malingering can be considered when a patient has been thoroughly assessed based on their history and physical examination (with appropriate diagnostic testing). Tools exist to help psychiatrists, neurologists and occupational physicians in diagnosing malingering, but these are largely out of the skill set of most emergency physicians. To determine if malingering should be suspected there are several questions to consider: are there any rewards the patient may be seeking after? What incentive may the patient have to seek after hospitalization, time off work, or addictive medication prescriptions? In most cases a team-based approach involving interdisciplinary professionals and sufficient collateral information are required to (1) make the diagnosis of malingering substantiated and (2) free from the excessive medicolegal risks of misdiagnosis. Emergency department clinicians must vigilantly consider malingering, factitious disorders, and other psychiatric illness as diagnoses of exclusion.

Chris Lipp, MD
Attending Physician
Calgary Emergency Medicine
Author at CanadiEM
Co-Founder of CRACKCast
How To Cite This Post
[Peer-Reviewed, Web Publication] Wibberley, A. Ray, K. (2020, Feb 24). Malingering in the ED. [NUEM Blog. Expert Commentary by Lipp, C]. Retrieved from http://www.nuemblog.com/blog/malingering
Other Posts You Might Enjoy…
Verbal De-escalation in the ED
Written by: Vidya Eswaran, MD (NUEM PGY-3), Zach Schmitz, MD (NUEM PGY-2), Abiye Ibiebele, MD (NUEM PGY-2) Edited by: Michael Macias, MD and Arthur Moore, MD (NUEM Alum ‘17) Expert commentary by: John Bailitz, MD
Introduction
I’ve been suffering in that waiting room for hours!
That worthless tech stabbed me with a needle ten times!!
If you don’t give what I want right now, I am going to hurt someone!!!
Every emergency physician can recall a time when they hear these words or similar phrases echoing throughout the Emergency Department (ED). As a patient becomes increasingly agitated, nearby staff and visitors become distracted, and ultimately concerned about everyone’s safety. Emergency Physicians can help restore the calm amidst the chaos by recognizing subtle clues and intervening early.
According to the Bureau of Labor Statistics, those who work in the healthcare sector had three times the rate of illness and injury from violence compared to all private industries [1]. In a survey of emergency medicine residents, 65.6% reported an experience of physical violence by a patient, 96.6% reported verbal harassment from a patient, and 52.1% reported sexual harassment by a patient. Often these patients were under the influence of drugs or alcohol, had a psychiatric disease, or an organic cause of their agitation, such as dementia [2]. In Australian emergency departments, 3 of every 1000 ED visits are associated with an episode of violence or acute behavioral disturbance [3].
When violence by a patient is imminent or has already occurred, the patient requires immediate restraint by either chemical or physical means [4]. ACEP guidelines for patient restraints supports the careful and appropriate use of restraints or seclusion if “careful assessment establishes that the patient is a danger to self or others by virtue of a medical or psychiatric condition and when verbal de-escalation is not successful [5].” Verbal “de-escalation techniques aim to stop the ascension of aggression to violence, and the use of physically restrictive practices, via a range of psychosocial techniques [6],” and should be tried before one simply grabs “5 and 2.”
Clinical Approach to Agitation
How do you determine which patients would benefit from verbal de-escalation?
Look for the agitated patient, the one who has an angry demeanor, using loud and aggressive speech, seems tense and is grasping their bed rails or clenching their fists, the one who is pacing or fidgeting [4]. These patients are in the pre-violent stage, and may have the potential to be successfully talked down. If a patient has already engaged in violent acts, it is too late to intervene with verbal de-escalation methods.
What principles should be used to assist with verbal de-escalation of the agitated patient?
In 2012 the American Association for Emergency Psychiatry offered a consensus statement on verbal de-escalation and created ten key domains to guide care of agitated patients. These domains offer a great framework for how to approach the agitated patient before the situation escalates [7].
Domain 1: Respect the patient’s and your personal space. First and foremost in any patient encounter, especially one with an agitated patient, is your safety. Aim to keep at least 2 arms lengths distance between you and the patient. This offers you room for your own personal safety, and is seen as non-confrontational and non-threatening in the eyes of the patient. Ensure that both you and the patient have an unobstructed pathway to the exits and that you do not stand in the way of the patient’s path to leaving the room.
Domain 2: Do not be provocative. The majority of our interpersonal interactions is communicated not by the words we say, but how we say them. Our body language is crucial and we must be mindful of it when attempting to calm a patient. Keep your hands visible and at ease, bend your knees slightly, avoid excessive direct eye contact and approach your patient from an angle instead of head-on. These positions convey a non-threatening demeanor.
Domain 3: Establish verbal contact. The first person to interact with the patient should be the one who leads the verbal de-escalation. Introduce yourself and tell the patient your role and orient them to their surroundings. Then, ask the patient what they would like to be called. This gives the patient the impression that you believe he or she is important and has some control over the situation.
Domain 4: Be concise and caring. Use short sentences and simple vocabulary to get your point across. Give your patients time to process what you have said and to respond before continuing. You should be prepared to repeat your message multiple times until your patient understands.
Domain 5: Identify wants and feelings. In order to provide empathetic care, you must understand your patient’s perspective. Listen carefully to what your patient says to pick up clues and respond to their desires. One tactic is to say “I really need to know what you expected when you came to the ED today. Even if I can’t provide it, I would like to know so that we can work on it together.”
Domain 6: Listen closely to what the patient is saying. This is closely related to Domain 5. Practice closed loop communication, repeat what the patient has told you to ensure you have understood them correctly.
Domain 7: Agree, or agree to disagree. Look for something that you can agree with in what the patient is saying. “I agree, waiting can be frustrating” or “Yes, I understand that the nurse has stuck you three times.” However, if you can’t find something to agree with the patient about, do not lie - agree to disagree.
Domain 8: Lay down the law and set clear limits. Draw a line which the patient must not cross. Let him or her know that harming himself or others is unacceptable and will result in specific consequences (seclusion, arrest, prosecution). This should not be portrayed as a threat, but rather be conveyed in a respectful manner. You can preface it with “Your behavior is making our staff uncomfortable and that makes it difficult for us to help you.”
Domain 9: Coach the patient on how to stay in control. Give the patient tactics they can use to help de-escalate the situation. “If you sit down we can discuss why you are here.”
Domain 10: Be optimistic and provide hope that the patient will be able to get to a favorable outcome. “I don’t want you to stay here longer than you need to. Let’s work together to help you get out of here feeling better.” Be sure to debrief with the patient and staff after the de-escalation, so that there is a strategy in place if this were to happen again.
Other strategies include recruiting the patient’s friends and family to help and to employ the three Fs technique - feel, felt, found [8]. “I understand that you feel X. Others in the same situation have felt that way to. Most have found that doing Y can help [4].”
Think of verbal de-escalation as a procedure just like intubations or central lines - with practice, comes mastery. Rehearse what you plan to say, and do mental run-throughs of de-escalations. Watch and learn from others who do this well. The English Modified De-Escalating Aggressive Behaviour Scale (EMDABS) is a validated tool you can use to assess your performance during de-escalations [9].
Summary
Unfortunately, physical and chemical restraint of the severely agitated patient is sometimes needed to protect ED staff, visitors, and the patient themselves. [10,11]. But by recognizing subtle signs of agitation early, we can often utilize effective verbal-de-escalation techniques to create safety for everyone!
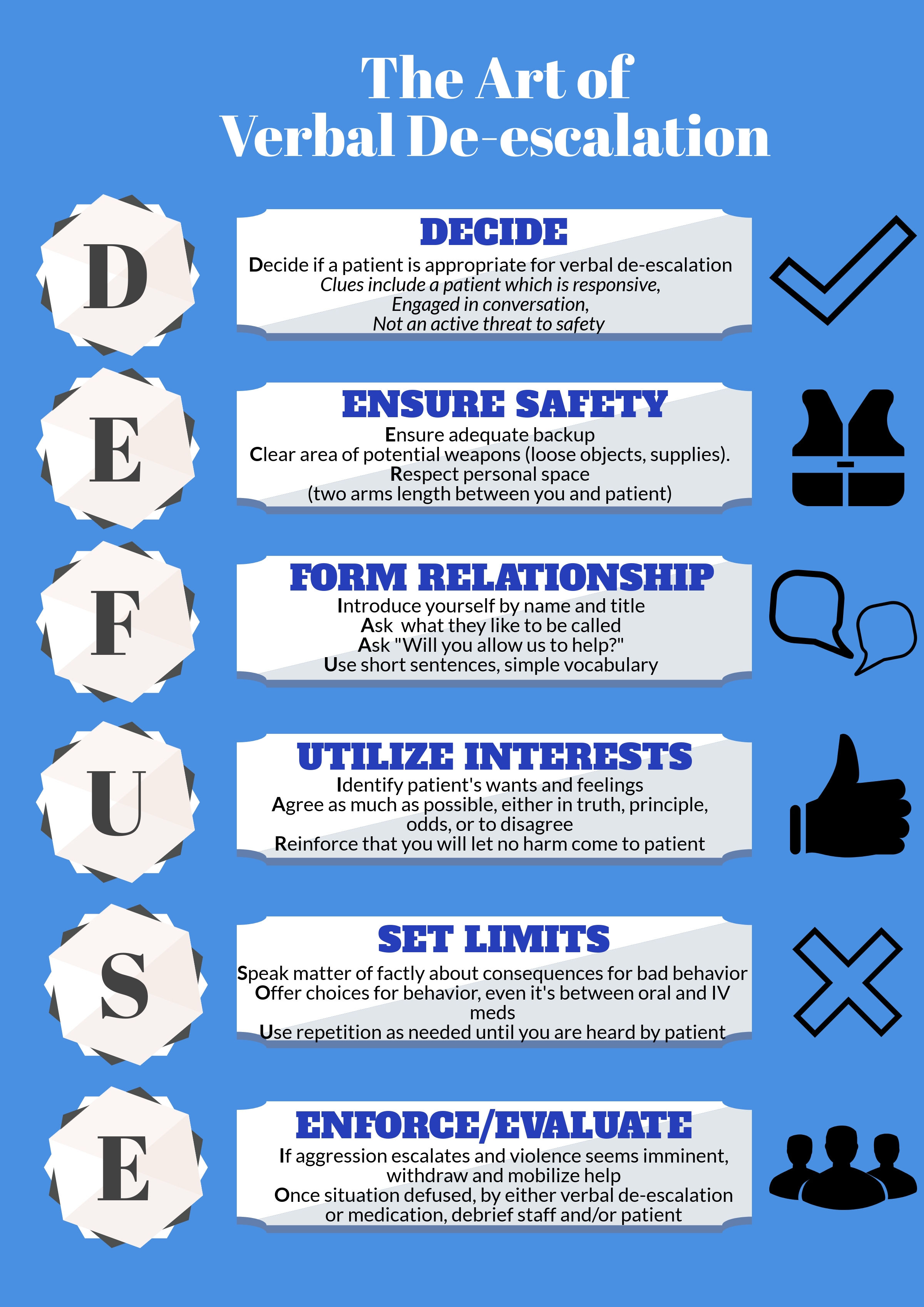
Check out our infographic for an easy to use mnemonic which summaries key points.
Expert Commentary
Thank you for this outstanding review of an incredibly important topic topic with tragically little supporting evidence to guide best practice. Colleagues and patients in multiple different practice settings throughout Chicago have repeatedly taught me several key pearls and pitfalls when dealing with the agitated patient.
For the mildly agitated patient, always open with an apology that empathically validates the patient or visitor emotions. “I am very sorry that you have been suffering in the waiting room for so long. That must have been very frustrating. My sincere apologies.” Never reply with a sharp justification or any explanation. Just acknowledge their frustration, own it, and the patient will quickly move past the emotion. Often times, this first connection forms the foundation of a healthy patient physician relationship and even a thank you letter to your ED Director.
For the patient whose agitation is escalating despite appropriate efforts by trained ED staff, call security or hit the duress button for back up before stepping into any potentially risky situation. If you are single covered at 3 AM, you cannot become another patient. When help arrives, ask security to simply stand in the hallway as you begin your DEFUSE techniques. Politely but purposefully excuse inexperienced staff members who have themselves become agitated and entered into a shouting match with patients or visitors. Always keep your own emotions in check and debrief with everyone involved after each learning opportunity.
Finally, when the sedation is needed for patient and staff safety, assemble your team, and proceed with the utmost professionalism. As a physician, you have no role in the physical restraint process unless absolutely necessary. Your security staff has been trained in proper physical restraints while chemical sedation catches up with the dangerous patient. If the patient is acutely agitated without concerns for respiratory depression, utilize 5 mg of Haldol + 5 mg of versed instead of the traditional 2 mg of Ativan. Everyone in the ED will become safer more quickly and the patient will wake up more rapidly for reassessment.
Just remember, “Patients First” always starts with everyone’s safety first!

John Bailitz, MD
Program Director, Northwestern Emergency Medicine
How To Cite This Post
[Peer-Reviewed, Web Publication] Eswaran V, Schmitz Z, Ibiebele A, Macias M, Moore A. (2019, March 4). Verbal De-escalation in the ED. [NUEM Blog. Expert Commentary by Bailitz J]. Retrieved from http://www.nuemblog.com/blog/verbal-deescalation
Other Posts You May Enjoy


References
Nonfatal Occupational Injuries and Illnesses Requiring Days Away From Work, 2014.Bureau of Labor and Statistics News Release. 2015. http://www.bls.gov/news.release/archives/osh2_11192015.pdf
Schnapp et al. Workplace Violence and Harassment Against Emergency Medicine Residents, WJEM 2016: 17(5) 567-573. https://www-ncbi-nlm-nih-gov.ezproxy.galter.northwestern.edu/pmc/articles/PMC5017841/pdf/wjem-17-567.pdf
Downes et al. Structured team approach to the agitated patient in the emergency department. Emergency Medicine Australasia (2009) 21, 196-202 http://onlinelibrary.wiley.com.ezproxy.galter.northwestern.edu/doi/10.1111/j.1742-6723.2009.01182.x/epdf
Moore, G and Pfaff, J. Assessment and emergency management of the acutely agitated or violent adult.Up to Date. https://www-uptodate-com.ezproxy.galter.northwestern.edu/contents/assessment-and-emergency-management-of-the-acutely-agitated-or-violent-adult?source=search_result&search=Assessment%20and%20emergency%20management%20of%20the%20acutely%20agitated%20or%20violent%20adult&selectedTitle=1~150#H17
ACEP Policy on Patient Restraints https://www.acep.org/Clinical---Practice-Management/Use-of-Patient-Restraints/
Price et al. Learning and performance outcomes of mental health staff training in de-escalation techniques for the management of violence and aggression. The British Journal of Psychiatry (2015) 206, 447-455 http://bjp.rcpsych.org.ezproxy.galter.northwestern.edu/content/bjprcpsych/206/6/447.full.pdf
JS Richmond et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health 2012: 13(1) 17-25. http://escholarship.org/uc/item/55g994m6
Nickson, C. De-Escalation. Life in the Fast Lane. 2014. http://lifeinthefastlane.com/ccc/de-escalation/
Mavandadi et al. Effective ingredients of verbal de-escalation: validating an English modified version of the ‘De-Escalating Aggressive Behaviour Scale’. Journal of Psychiatric and Mental Health Nursing, 2016, 23, 357-368. http://onlinelibrary.wiley.com.ezproxy.galter.northwestern.edu/doi/10.1111/jpm.12310/epdf
Weingart, S. Podcast 060 – On Human Bondage and the Art of the Chemical Takedown. EMCrit. 2011. http://emcrit.org/podcasts/human-bondage-chemical-takedown/
Nickson, C. Chemical Restraint. Life in the Fast Lane. 2014. http://lifeinthefastlane.com/ccc/chemical-restraint/