

Indications and steps for performing delayed sequence intubation
Posts tagged #intubation
C-Spine Intubation

Written by: Daniel Levine, MD (NUEM ‘24) Edited by: Zach Schmitz (NUEM ‘21)
Expert Commentary by: Matt Levine, MD
The “Evidence” Behind Manual In-Line Stabilization During Intubation of Trauma Patients
Background
Even in the absence of frank head and neck trauma that may cause bleeding or distortions in usual anatomy, trauma patients present challenging airways because of cervical spine precautions. Standard-of-care technique according to EAST (Eastern Association for the Surgery of Trauma), West (Western Trauma Association), and ATLS (Advanced Trauma Life Support) guidelines for intubating acute trauma patients with known or potential cervical spine injury involves manual in-line stabilization (MILS). (1,2) This is a two-person technique whereby one provider performs laryngoscopy while another holds the patient’s neck in place. The two most common techniques for this procedure are depicted below, one in which the stabilizer crouches down at the head of the bed (A), and the other where the stabilizer approaches from the side of the bed (B). (3)
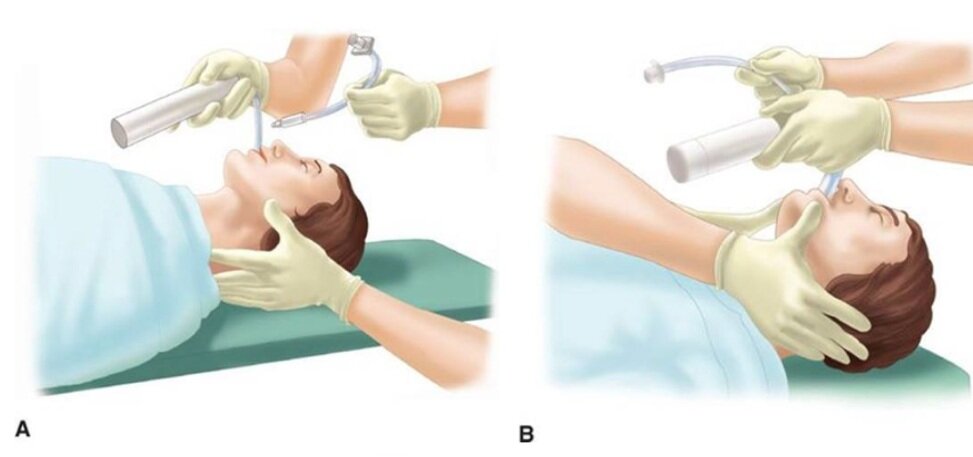
(photo from Strange and Schafermeyer's Pediatric Emergency Medicine, 4th edition) (3)
Evidence
Like many practices in medicine, MILS has never been studied in randomized controlled trials, and the practice stems more from weak data and expert opinion. (4) The practice of spinal stabilization began during the 1970s after a retrospective review published in 1979 of 300 patients with acute cervical injuries who presented to Johns Hopkins hospital between 1950 and 1972. Although the main focus was on the effects of laminectomy and steroids, the review also found that 11 of the 300 patients developed neurologic deficits after reaching the hospital. Of the 11 patients, 7 developed these deficits “after neck immobilization was not provided”, with no clear comment as to whether immobilization was not provided during intubation or during some other process of the patient’s care. (5) These observations led to concerns that mobilization of the neck during intubation may worsen spinal cord injury, so manual in-line stabilization became standard of care in the 1980s.
Existing data for spinal stabilization comes from trials of cadaveric models, case series, and uninjured patients. Data from cadavers with post-mortem surgically created cervical spine injuries have shown mixed results on the effects of the amount of measured movement at the injured site with versus without MILS. For example, a 1993 study by Donaldson et al. found higher degrees of subluxation and angulation at C5-C6 during orotracheal intubation without MILS compared to with stabilization in five cadaveric specimens with injuries created in that area. (6) On the other hand, a 2001 Lennarson et al. study on cadavers found MILS significantly increased subluxation in C4-C5 during the same movements. (7) While it is somewhat counterintuitive that performing MILS might be associated with increased cervical motion, this may be explained by the laryngoscopist’s need to apply greater force with the laryngoscope in order to obtain an adequate view. This is what Santoni et al. (2009) found in a matched control study of 9 patients undergoing elective surgery. The patients in this study underwent two sequential laryngoscopies and oral intubations with a Macintosh 3 blade. Pressure transducers attached to the end of the blades detected higher maximum pressures at best glottic view with MILS compared to without. (8)
What is more clear in the literature on MILS than its effect on cervical motion is that it impairs glottic visualization and subsequent first pass intubation success. In the aforementioned Donaldson study on cadavers, MILS was shown to have a negative impact on Cormack-Lehane (CL) grade. (6) Similarly, in the aforementioned Santoni et al. study of 9 patients who underwent two sequential intubations with and without MILS, glottic visualization was worse in 6 patients with MILS, and intubation failure occurred in 2 of these 6 patients compared to no intubation failures among these patients when the intubation was performed without MILS. Thiboutot et al. (2008) performed a randomized controlled trial that further demonstrated this effect. In their study, 200 elective surgical patients were randomized to receive MILS or no MILS, and the primary endpoint was rate of failed intubation at 30 seconds with a Mac 3 blade. The rate of failed intubation was half in the MILS group (50%, 47/94), significantly higher compared to the control group (5.7%, 6/105). When they released manual in-line stabilization, they were able to intubate all patients. Secondary outcomes of rate of CL grade 3-4 as well as mean latency to successful intubation were also both significantly higher in the MILS group. (9) Additionally, these data were from patients undergoing elective surgery being intubated in the controlled OR setting by anesthesiologists. It is likely that the rate of failed intubation would be even higher in the chaotic emergency department environment with an acutely injured trauma patient. While 30 seconds is a somewhat arbitrary cutoff for a failed intubation, and it is quite possible many of the patients in the MILS group who “failed” may have been successfully intubated if a longer cut-off time were chosen, hypoxia caused by failed or delayed intubation is associated with poor outcome in central nervous system injury. (10)
Conclusion
In an ideal world, a large-scale randomized controlled trial of trauma patients studying the effects of MILS on mortality and important functional neurologic outcomes would help elucidate the utility of this commonly accepted practice. However realistically, completing such a study has significant obstacles. Cervical spine injuries are relatively rare (4% of trauma injured patients)4 and only a small fraction of those cases involve unstable injuries with potentially salvageable cord function. Thus, a study with sufficient power to detect any meaningful difference in outcomes would take many thousands of patients, many trauma centers, and many years to complete. Perhaps an even larger hurdle is the ethical and medicolegal hurdle of randomizing patients to not getting MILS and possibly putting them at risk of quadriplegia. (4) So what’s a clinician to do when faced with the common scenario of having to intubate a trauma patient? I personally like the approach that Dr. Reuben Strayer discusses in his video “Advanced Airway Management for the Emergency Physician” (link below). (11) To summarize his strategy:

*The exception: in the rare situation where the patient has a highly suspected (e.g. obvious bony deformity, focal neurologic deficit) or known cervical spine injury, Dr. Strayer recommends lowering the threshold to perform a cricothyroidotomy. Additionally, he recommends considering an awake intubation approach in these patients.
Another consideration is intubating using a hyper-angulated video GlideScope, which has been shown to have improved CL views and high rates of intubation success in c-spine immobilized patients. (12) That said, occasionally equipment availability or a bloody airway may preclude the use of video laryngoscopy in the trauma setting.
References
Mayglothling J, Duane TM, Gibbs M, McCunn M, Legome E, Eastman AL, Whelan J, Shah KH; Eastern Association for the Surgery of Trauma. Emergency tracheal intubation immediately following traumatic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012 Nov;73(5 Suppl 4).
Brown CVR, Inaba K, Shatz DV, Moore EE, Ciesla D, Sava JA, Alam HB, Brasel K, Vercruysse G, Sperry JL, Rizzo AG, Martin M. Western Trauma Association critical decisions in trauma: airway management in adult trauma patients. Trauma Surg Acute Care Open. 2020 Oct 9;5(1)
Leonard, J et al. "Strange and Schafermeyer's Pediatric Emergency Medicine, 4th edition." Chapter 24: Cervical Spine Injury. https://doctorlib.info/pediatric/schafermeyers-pediatric-emergency-medicine/24.html, accessed 5/7/21.
Manoach S, Paladino L. Manual in-line stabilization for acute airway management of suspected cervical spine injury: historical review and current questions. Ann Emerg Med. 2007 Sep;50(3):236-45.
Bohlman HH. Acute fractures and dislocations of the cervical spine. An analysis of three hundred hospitalized patients and review of the literature. J Bone Joint Surg Am. 1979;61:1119- 1142.
Donaldson WF 3rd, Towers JD, Doctor A, et al. A methodology to evaluate motion of the unstable spine during intubation techniques. Spine. 1993;18:2020-2023
Lennarson PJ, Smith DW, Sawin PD, Todd MM, Sato Y, Traynelis VC. Cervical spinal motion during intubation: efficacy of stabilization maneuvers in the setting of complete segmental instability. J Neurosurg. 2001 Apr;94(2 Suppl):265-70.
Santoni BG, Hindman BJ, Puttlitz CM, Weeks JB, Johnson N, Maktabi MA, Todd MM. Manual in-line stabilization increases pressures applied by the laryngoscope blade during direct laryngoscopy and orotracheal intubation. Anesthesiology. 2009 Jan;110(1):24-31.
Thiboutot, F et al. Effect of manual in-line stabilization of the C-spine on the rate of difficult orotracheal intubation by direct laryngoscopy; a randomized controlled trial. Can J Anaesth. 2009 Jun;56(6):412-8.
Chesnut RM, Marshall LF, Klauber MR, Blunt BA, Baldwin N, Eisenberg HM, Jane JA, Marmarou A, Foulkes MA. The role of secondary brain injury in determining outcome from severe head injury. J Trauma. 1993 Feb;34(2):216-22.
“Advanced Airway Management for the Emergency Physician”, uploaded by Reuben Strayer, https://vimeo.com/12440392
Bathory I, Frascarolo P, Kern C, Schoettker P. Evaluation of the GlideScope for tracheal intubation in patients with cervical spine immobilisation by a semi-rigid collar. Anaesthesia. 2009 Dec;64(12):1337-41.
Expert Commentary
So once again a review of a significant body of literature leaves a clinical question unanswered, leaving the practitioner to either follow dogma or make one’s own conclusions. Like most of our medical decision making, this is a risk/benefit analysis. So let’s go through the process.
Some background context to keep in mind:
Most cervical spine injury occurs from the initial traumatic event (primary neurologic injury). Secondary neurologic injury is a cascade of events at the cellular level that worsen primary injury and is exacerbated by hypoxia and hypercarbia, which are frequent events in difficult/prolonged intubations. These must be minimized when the brain or c spine are injured!
The movements of the cervical spine that occur during ED care pale in magnitude to the cervical spine motion that caused the primary injury to occur. These likely contribute less to neurologic outcome than secondary neurologic injury from other events during ED care like hypotension, hypoxia, and hypocarbia.
It’s too difficult to intubate with a collar on. It must be carefully and temporarily removed. As Dr. Levine taught us, MILS impairs glottic visualization and first pass intubation success. Dr. Levine also taught us that we don’t know whether the injured cervical spine actually moves less or more with MILS during intubation attempts.
The synthesis:
These factors all lead me to agree with Dr. Strayer’s approach. It is reasonable to minimize cervical spine motion as much as possible, but not at the expense of adequate glottic visualization. Maybe MILS helps minimize motion during intubation. But abandon MILS when glottic visualization is suboptimal because MILS can be contributing to this, leading to hypoxia, hypercarbia, and secondary neurologic injury. Practice MILS only until it is possibly prolonging airway success, because now it is more likely to be harming than helping.
Even more future questions remain. Much of the prior literature is based on use of traditional orotracheal intubation techniques. How much of that knowledge applies to the now widespread use of fiberoptic video intubations (i.e. Glidescope), which may have better first pass success rates and less neck motion? Do we even need to perform MILS for these intubations? Or can we reliably rapidly intubate with MILS and the Glidecope – so we can have our cake and eat it too?

Matthew Levine, MD
Associate Professor of Emergency Medicine
Department of Emergency Medicine
Northwestern Memorial Hospital
How To Cite This Post:
[Peer-Reviewed, Web Publication] Levine, D. Schmitz, Z. (2021, Oct 18). C-Spine. [NUEM Blog. Expert Commentary by Levine, M]. Retrieved from http://www.nuemblog.com/blog/cervical-spine-intubation
Other Posts You May Enjoy







Awake Intubation

Written by: Patricia Bigach MD, (NUEM ‘23) Edited by: Terese Whipple (NUEM ‘20) Expert Commentary by: Seth Trueger MD, MPH

Expert Commentary
Awake intubation can sound imposing but simply means the patient is still breathing on their own. It is mostly just a matter of using topical lidocaine instead of paralyzing, and sedating the patient a bit to tolerate it. It will almost always require some sedation – ketamine procedural sedation works very well as the patient’s protective reflexes will be intact (until we topicalize) as will their respiratory drive.
It does not take long! Just spray lido instead of pushing NMBA. This is the key concept. If time is really a factor, I atomize the larynx, push ketamine, and then reload and spray more lidocaine as I do laryngoscopy; everything else is just like every other ED intubation.
Glycopyrrolate is nice but if it’s not handy, not worth a delay.
I find nebulizing doesn’t add much, mostly just gets the mouth. I still nebulize if I can get it set up quickly while prepping everything else (and it can help tolerate the atomizer).
Small touches of propofol might help relax the ketamine-sedated patient as well, including spontaneous/dissociated movements and tightly closed mouths. Dexmedetomidine might not be fast enough for ED intubations.
I usually use hyperangulated VL (eg Glidescope S3) – we are usually doing this for predicted difficult intubation, and now not optimizing intubating conditions. Fiberoptic requires a fair amount of skill and time. One of the main things that demystified awake intubation for me is it is a medication choice; it doesn’t always mean awake-fiber optic.
In non-COVID times, I would keep the nasal cannula on at 5-15lpm to keep the patient as oxygenated as possible, which is even better than during RSI because they’re still breathing, now with extra oxygen.
The paradox of awake intubation is that we take the patients we predict to be the most difficult anatomically, and then don’t optimize intubating conditions (no NMBA). Part of the beauty of awake intubation is that we also gain a ton of information even if unsuccessful without losing much; if I get a partial view in non-NMBA circumstances I can make a judgment call about proceeding to paralysis (ie RSI) or calling for help, etc.
Sedation-only or ketamine-only intubation can sound like a good idea but neither makes sense to me. It takes a lot of sedation to knock out protective airway reflexes to allow laryngoscopy, i.e. enough to impair respiratory drive. Topicalization is not hard with atomizers. Similarly, ketamine keeps the airway reflexes intact, which is why it is so safe for procedural sedation, so hard to imagine that laryngoscopy won’t be an issue.

Seth Trueger, MD, MPH
Assistant Professor of Emergency Medicine
Department of Emergency Medicine
Northwestern University
How To Cite This Post:
[Peer-Reviewed, Web Publication] Bigach, P. Whipple, T. (2021, Aug 20). Awake Intubation. [NUEM Blog. Expert Commentary by Trueger, S]. Retrieved from http://www.nuemblog.com/blog/awake-intubation
Other Posts You May Enjoy



Intubating the Pregnant Patient in the ED
Written by: Priyanka Sista, MD (NUEM ‘20) Edited by: Steve Chukwulebe, MD (NUEM ‘19) Expert Commentary by: Samir Patel, MD


Expert Commentary
Tip for #1 - While 3-5 minutes of 100% oxygen is ideal to achieve denitrogenation, in an emergency 8 vital capacity breaths (maximal inhalation and exhalation) with a high FiO2 source is sufficient in a cooperative patient.
Tip for #2 - Airway edema is even worse in preeclamptic patients, and Mallampati scores acutely worsen DURING labor. Don’t bother with direct laryngoscopy and go straight to the video laryngoscope if it’s available.
Tip for #3 - In this scenario, the ideal LMA or supraglottic airway is one that includes a port for passage of an OG tube. Your pregnant patient in the ER with increased aspiration risk is not likely to be NPO for 8 hours like they are for anesthesiologists before surgery.
Tip for #4 - The rapid sequence dose of rocuronium is 1.2 mg/kg. You can immediately reverse rocuronium with sugammadex 16 mg/kg if necessary. For cost purposes, succinylcholine is still the best choice unless medically contraindicated.
Tip for #5 - According to ACOG, if cardiac arrest occurs in a woman greater than 23 weeks gestation, and there is no return of spontaneous circulation after 4 minutes of correctly performed CPR, a perimortem c-section should be performed with the goal of delivering the fetus by the fifth minute.

Samir K. Patel, MD
Assistant Professor
Northwestern University Feinberg School of Medicine
Department of Anesthesiology
How To Cite This Post:
[Peer-Reviewed, Web Publication] Sista, P. Chukwulebe, S. (2021, Jan 18). Intubating the pregnant patient in the ED. [NUEM Blog. Expert Commentary by Patel, S]. Retrieved from http://www.nuemblog.com/blog/intubating-the-pregnant-patient.
Other Posts You May Enjoy





Physiologically Difficult Intubations
Written by: Samantha Stark, MD (NUEM ‘20) Edited by: Steve Chukwulebe, MD (NUEM ‘19) Expert Commentary by: Seth Trueger, MD, MPH
It’s the first few minutes of your shift, and the paramedics roll by your workstation with your first patient, a young woman clutching an inhaler and breathing with every accessory muscle in her body. You direct them to your resuscitation room and they inform you that she has a history of asthma and is having an attack; she’s too exhausted from breathing to verify this, but it seems true. You quickly get her on BiPAP, which mildly improves her work of breathing, but as she becomes drowsy, you obtain a VBG showing a climbing CO2 of 45. You realize that it’s time to intubate this patient, and as you get set up, you collect your thoughts and quickly review everything you’ve heard about intubating asthmatics.
Obstructive Airway Disease
First, remember that asthma is an obstructive airway disease, meaning that there are two main processes to worry about during and after intubation:
Auto PEEP
Hypotension secondary to increased intrathoracic pressure from auto PEEP
*Note: auto PEEP is caused by breath stacking in a patient whose expiration is impaired (such as asthma or COPD) – the ventilator initiates a breath before there’s time for full exhalation, and this leads to progressively more volume retained in the lungs, increasing the risk of barotrauma. This can also lead to increased intrathoracic pressure, in turn decreasing preload to the heart and thus causing hypotension.
How to optimize the intubation:
As you already have this patient on BiPAP, try to preoxygenate as much as possible with this mode of positive pressure
Consider attempting delayed sequence intubation with ketamine
It will maintain the patient’s respiratory drive and may help with BiPAP synchrony and anxiolysis
It serves as a bronchodilator
Use rocuronium for paralysis
It will last longer than succinylcholine, and initially help with vent synchrony
*Note: remember to fully sedate the patient after intubation, as they won’t tell us that they’re not sedated during their prolonged paralysis
Decrease the dead space and resistance of your vent by using the largest endotracheal tube feasible
Frequently reassess the ventilator to ensure that breath stacking is not occurring:
Low respiratory rate to allow for exhalation
Higher tidal volumes of 6-8 cc/kg IBW
Decreased I:E ratio (at least 1:3, may very well need to be longer)
You’ve successfully intubated this patient, and now the lab pages you to let you know that there is a patient in the waiting room with a bicarb of 9. When the patient is wheeled back, his marked tachypnea and work of breathing makes you think he may need to be intubated as well. But he’s so acidotic, and you’re sure you’ve hear something about intubating acidotic people…
Metabolic Acidosis
What you’ve heard is that if you intubate a severely acidotic patient, you’ve killed them. There are two reasons for this:
It’s very difficult to keep up with their minute ventilation
There is a transient increase in pCO2 with paralysis (this is normally inconsequential, but in the decompensating acidotic patient, can lead to cardiovascular collapse)
How to optimize the intubation:
Optimize cardiovascular status as much as possible beforehand
Bolus fluids
Consider starting pressors pre-intubation, or having push-dose phenylephrine or epinephrine on hand during intubation
Match the patient’s minute ventilation
Ensure adequate pre-oxygenation, using NIPPV
However, even if oxygenation is not an issue, BiPAP should be used to assess the minute ventilation the patient is maintaining on their own, to help determine what is needed post intubation
Using delayed sequence technique with ketamine as the induction agent and a short acting paralytic like succinylcholine could theoretically help to avoid apnea as much as possible
Once intubated, the patient’s pre-intubation minute ventilation (respiratory rate and tidal volume) MUST be matched on the ventilator
Don’t be surprised to see higher tidal volumes of 8 cc/kg IBW
As you’re sitting down to catch up on notes, a nurse gets your attention to let you know that there is an altered, febrile, tachycardic patient with a pressure of 65/40 tucked away in a bed at the back of the ED that you should probably see right away. As it turns out, this patient needs to be intubated as well.
Shock
As mentioned above, increased intrathoracic pressure from PPV results in decreased venous return to the heart, leading to decreased preload. This obviously has the potential to be quite detrimental to a patient with shock.
How to optimize the intubation:
Optimize cardiovascular status as much as possible beforehand
Fluid resuscitation and vasopressors started prior to intubation
Have push dose pressors available at the bedside should they be needed
Induction agents:
Avoid propofol as it has a propensity to cause hypotension
Use etomidate or ketamine
Ketamine has been shown to be more hemodynamically stable than etomidate
Also, the body should prioritize cerebrovascular blood flow in shock, therefore if etomidate is used, consider decreasing the dose to minimize hemodynamic effects
At this point, you’re too tired to write any notes, so you decide to sit down and, given how your shift has been going so far, do some reading about patients that are dangerous to intubate or difficult to manage on the vent. The first topic you come across is pulmonary hypertension.
Pulmonary Hypertension
Mechanical ventilation is dangerous in these patients due to their inability to tolerate decreased preload, increased afterload, or really any alteration in their tenuous hemodynamics. Unfortunately, in patients with pulmonary hypertension but also systemic hypotension, IV fluids can over-distend the right ventricle and make things worse. There’s not a super reliable way to tell if these patients will be fluid responsive or not; most would suggest a small fluid bolus challenge to see how they respond. There may or may not be time for this prior to intubation, but if there is time, it’s probably worth a try.
How to optimize the intubation:
Can consider pre-medication with fentanyl:
Thought to blunt the hypertensive response to laryngoscopy, similar to head-injured patients
In theory, this prevents increased afterload in the pulmonary vasculature
Induction agent:
Consider etomidate
Theoretically should have less of an effect on preload than propofol
Additionally, less of an effect on afterload than ketamine
Ventilator settings:
Closely monitor plateau pressures to keep them less than 30 cm H2O, to avoid drops in preload due to increased intrathoracic pressure
Consider placing an arterial line for frequent ABG checks
Both hypercapnia and hypoxia can cause vasoconstriction (increasing afterload in the pulmonary vasculature)
Two days later, while you’re following up on some of your prior patients, you note that the patient in septic shock that you intubated a couple of days ago now has ARDS, and it seems that the inpatient team is having some difficulty managing her on the vent.
ARDS
While this is an area of active research and there are different strategies and methods for helping to improve these patients’ oxygenation, the main thing to remember from the perspective of managing the ventilator is the lung protective strategy:
Tidal volume 6 cc/kg IBW
Plateau pressure less than 30 cm H2O
Minimum PEEP of 5 cm H2O (and remember that these patients may often need significantly higher PEEP)
Expert Commentary
Thank you for this review of intubating sick patients - intubating complex physiology is arguably one of the most dangerous things we can do, but there are some straightforward, concrete steps we can take to do it as safely as possible.
For me, the first step is to consider every ED intubation potentially dangerous. Maximize resuscitation (IV fluids; pressors if needed, always ready) and optimize preoxygenation to provide the biggest possible safety net. It’s much more CBA than ABC.
Every patient we intubate in the ED has potential to crump: the sympatholysis from sedation will reduce endogenous catecholamines, and the switch to positive pressure ventilation impairs preload.
Every intubated patient needs post-intubation sedation. I generally default to a fentanyl drip and modify from there (eg add propofol if BP tolerates; add ketamine if not). Do not remove sedation for hypotension; do not use pain as a pressor. That is torture and it is bad. Sedate the patient adequately and if that means more resuscitation (fluid, blood, pressors, etc) then do that too. Do not torture patients to maintain BP.
The easiest tactic to ensure post-intubation sedation is to think of RSI as 3 medications: NMBA, induction agent, and post-intubation sedative. I should not be surprised that I will need post-intubation sedation shortly after intubation.
Perhaps the biggest lesson in ARDS management and prevention in recent years is that nearly everyone potentially benefits from lung protective ventilation, i.e. 6 ml/kg *ideal* body weight. I’ve changed my default tidal volume to 400-450ml (it was 550-600 when I was in med school). Otherwise, ventilation (minute ventilation, or CO2 management) is all about adjusting respiratory rate (my default is 16-18, not 12) as the patient’s height usually does not change in the ED.
Special situations: asthma patients don’t have a big enough tube to exhale properly. Pay special attention, make sure they have sufficient time to exhale (and they may the one group that may benefit from *not* being on 6 ml/kg IBW. Perhaps even more importantly, unlike many other situations, intubation does not fix asthma; it makes it even harder to manage, as even the largest ET tubes are, by definition, smaller than the patient’s natural airway. Maximize NIV and other management options (eg epinephrine) if at all possible.
Acidosis is tough and the key is maximizing ventilation before and after intubation. These patients may need absurd-seeming respiratory rates and regardless of how hypercarbic they are, acidosis does not make patients taller so there is no reason to adjust tidal volume.
Pulmonary hypertension is complex and scary. Prepare beforehand, and work with your intensivists and other relevant specialists.
The most important part of airway management is preparation – not just in the ED, but learning as much as I can beforehand.

Seth Trueger, MD, MPH
Assistant Professor of Emergency Medicine
Department of Emergency Medicine
Northwestern University expert commentator
How To Cite This Post:
[Peer-Reviewed, Web Publication] Stark, S. Chukwulebe, S. (2020, Oct 5). Physiologically Difficult Intubations. [NUEM Blog. Expert Commentary by Trueger, S]. Retrieved from http://www.nuemblog.com/blog/physiologically-difficult-intubations
Other Posts You May Enjoy
References
Ebert TJ, Muzi M, Berens R. Sympathetic responses to induction of anesthesia in humans with propofol or etomidate. Anesthesiology. 1992;76:725-33.
Van Berkel MA, Exline MC, Cape KM, et al. Increased incidence of clinical hypotension with etomidate compared to ketamine for intubation in septic patients: a propensity matched analysis. Journal of Critical Care. 2017;38:209-214.
Dalabih M, Rischard F, Mosier JM. What’s new: the management of acute right ventricular decompensation of chronic pulmonary hypertension. Intensive Care Med. 2014;40(12):1930-3.
Hemmingsen C, Nielson PC, Odorico J. Ketamine in the treatment of bronchospasm during mechanical ventilation. Am J emerg Med. July 1994;12(4):417-420.
Eames WO, Rooke GA, Wu RS, Bishop MJ. Comparison of the effects of etomidate, propofol, and thiopental on respiratory resistance after tracheal intubation. Anesthesiology. June 1996;84(6):1307-11.
Gragossian A, Asp A, Hamilton R. High Risk Post Intubation Patients. www.emdocs.net/ high-risk-post-intubation-patients/ June 2017
The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes fo acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301-1308.
NIH NHLBI ARDS Clinical Network. Mechanical Ventilation Protocol Summary. www.ardsnet.org/files/ventilator_protocol_2008-07.pdf
Marino, Paul L. 2009. The Little ICU Book. Wolters Kluwer Health. Philadelphia, PA.
Arbo, John E. 2015. Decision Making in Emergency Critical Care: An Evidence-Based Handbook. Wolters Kluwer Health. Philadelphia, PA.
The Top NUEM Blog Posts of 2019

Edited by: Maury Hajjar, MD (NUEM PGY-2), Niki Patel, MD (NUEM PGY-2), Vytas Karalius, MD, (NUEM PGY-2), Justine Ko (NUEM PGY-3) Expert commentary by: Seth Trueger, MD
Happy New Year, Everyone!
Let’s take a look back at the 2019 NUEM Blog!
The Top Ten NUEM Blog Posts of 2019
10. REBOA
Recent grads Andew Cunningham, Bill Burns, and Trauma/EM doc Zaffer Qasim walk us through the ever-popular and sublimely named REBOA.
9. The Seriousness of Deliriousness
Thorough discussion of the important but easy to overlook issue of delirium in the ED by Nery Porras, recent grad and current neuro critical care fellow Katie Colton and geriatrician Lee Lindquist.
8. Pelvic Fractures
Justine Ko, Terese Whipple, and Matt Levine walk is through pelvic fractures and the important associated injuries.
7. Verbal Deescalation in the ED
Vidya Eswaran, Zach Schmitz, Abiye Ibiebele, NUEM-blog-founder Michael Macias, recent grad Arthur Moore, and John Bailitz review the complex but important topic of verbal deescalation in the ED.
6. Visual Guide to Splinting
Recent grad and current Stanford med ed fellow, recentish grad John Sarwarkand remote grad Matthew Pirotte provide a surprising amount of information in a small amount of words & images.
5. Post-Intubation Management
It’s easy to fall into the trap getting the tube & high-fiving and walking away; Andra Farcas, recent grad and current Air Force doc Paul Trinquero and recentish grad Andrew Pirotte walk is through the steps to post-intubation management.
4. Flexor Tenosynovitis
Thorough and concise review of flexor tenosynovitis by Kevin Dyer and recent grad Adnan Hussain, featuring expert commentary hand surgeon Avi Giladi (who also had the #4 post in 2018).
3. Tetracaine
Nice review by Jonathan Hung and recent grad and current med ed fellow Matt Klein of an Annals study showing a safe approach to tetracaine for corneal abrasions. Won’t solve the controversy but does include an expert commentary by @DGlaucomflecken
2. Intubation Positioning: Beyond the Sniffing Position
Unfortunately, optimal positioning is not always optimally executed in the ED; this post reviews both “standard” sniffing position and ramping, which, if nothing else, will help push us to better position our patients. Very nice work by recent grad and current neuro critical care fellow Katie Colton, and recent grad Charles Caffrey, and recentish grad Andrew Pirotte!
1. Unstable C-Spine Fractures
The top spot goes to a very nice succinct review by recent grads Sarah Sanders and Alison Marshall featuring beautiful images and a commentary by NLFH faculty Steve Hodges.
How to cite this post
[Peer-Reviewed, Web Publication] Hajjar M, Patel N, Karalius V, Ko J, (2019, December 30 ). The Top NUEM Blog Posts of 2019. [NUEM Blog. Expert Commentary by Trueger S ]. Retrieved from http://www.nuemblog.com/blog/top-ten-2019.
Other posts you might enjoy…
Bougie Journal Club

Written by: Amanda Randolph, MD (NUEM PGY-3) Edited by: Katie Colton, MD (NUEM ‘19) Expert commentary by: Howard Kim, MD
Introduction:
Endotracheal intubation is one of the most common and life-saving procedures performed in the Emergency Department (ED), though it is not without risk – approximately 12% of ED intubations result in an adverse event. First-pass success has been linked to improved outcomes, but in the case of a difficult airway, this goal can be challenging. The bougie is typically reserved as a rescue device in these situations. However, a study recently published in JAMA questions this approach, and instead asks whether the routine use of a bougie during all difficult airway attempts would improve first-pass success.
The Study:
Driver BE, Prekker ME, Klein LR, et al. Effect of Use of a Bougie vs Endotracheal Tube and Stylet on First-Attempt Intubation Success Among Patients With Difficult Airways Undergoing Emergency Intubation: A Randomized Clinical Trial. JAMA. 2018;319(21):2179–2189. doi:10.1001/jama.2018.6496
Study Design:
This study was a randomized clinical trial performed at Hennepin County Medical Center, an urban academic Emergency Department.
Population:
Investigators enrolled consecutive patients 18 years and older whom the attending emergency physician planned to intubate using a Macintosh laryngoscope blade (direct or video).
Exclusion criteria included known anatomic distortion of the upper airway (ie angioedema, epiglottitis, laryngeal mass, or malignancy), as the bougie has already been proven more effective in these patients in previous studies. Prisoners and pregnant patients were also excluded.
After intubation, the physician recorded whether any difficult airway features were present: body fluids obscuring the laryngeal view, airway obstruction or edema, obesity, short neck, small mandible, large tongue, facial trauma, or cervical spine immobilization. Patients were then subcategorized based on the presence of 1 or more difficult airway characteristics.
Intervention Protocol:
To optimize a balanced study population, eligible patients were first sorted into 2 strata – those with obesity or cervical immobilization, and those without these features. From that point, patients from each stratum was randomized 1:1 to either bougie or endotracheal tube (ET tube) + stylet for the first attempt.
The intubating physician was free to direct the procedure as they saw fit, including patient positioning, pre-oxygenation, the use of RSI, and cricoid pressure. The physician could choose between direct laryngoscopy using a Macintosh blade, or video laryngoscopy using a C-MAC or GlideScope. If video laryngoscopy was chosen, the physician could elect whether to view the video screen.
In the bougie group, the physician inserted the bougie into the trachea, an assistant loaded the ET tube, and the operator guided the tube through the vocal cords. If resistance was met, the physician retracted the tube 2cm, rotated 90 degrees and re-advanced.
In the ET tube + stylet group, a straight to cuff shape was used. If resistance was encountered, the physician could reshape the tube/stylet as needed.
If intubation was unsuccessful on the first attempt, the physician was free to change any equipment or devices. Correct tube placement was determined by waveform capnography.
Outcome Measures:
Primary outcome: first-pass intubation success
Successful intubation on the first laryngoscopy attempt with device as previously randomized (bougie or ET tube)
Secondary outcomes:
Hypoxemia (sat < 90%, or > 10% desat during intubation if already hypoxemic)
First attempt time elapsed (laryngoscope insertion to removal)
Esophageal intubation
Results:
In patients randomized to the bougie arm, there was a 14% absolute increase in the rate of first-pass success in patients with at least one difficult airway feature (96% vs 82% bougie vs ET tube +stylet).
The bougie approach was superior in subsets of patients with predictors of airway difficulty including C-spine immobilization, obesity, and Cormak-Lehane grades 2-4.
Even in patients not predicted to have a difficult airway, there was a 7% absolute increase in first-pass success with the bougie approach (99% vs 92% with ET tube + stylet).
There was a small but significant increase in the time elapsed on first-pass success with the bougie (38 seconds) vs ET tube + stylet (34 seconds).
A more extensive summary of the results is depicted in Table 3:

Interpretation:
This study concludes that the bougie improves first-pass success rate both in difficult airways and standard airways. The small increase in time to first-pass success when using a bougie is outweighed by the need to fall back on rescue techniques more frequently when starting with an ET tube and stylet. Therefore, authors propose the use of a bougie as a routine primary intubation device for all patients. This argument is compelling and potentially practice-changing. Most EDs including NMH have adopted the practice of using a bougie right away when there is an obviously difficult airway (laryngeal mass, neck hematoma etc), but otherwise the bougie is often reserved for backup after one or more failed attempts. This relies on a perhaps now invalid model of an algorithmic approach to the difficult airway in which operators progress through a series of rescue devices and maneuvers. In light of this study, it may be time for a culture shift in EM toward routine bougie use.
Strengths:
This is a well-designed randomized controlled trial, with a total of 752 patients studied, generating enough power to provide meaningful results. The methodology of using the bougie and the ET tube + stylet was highly standardized. At the same time, the physicians were free to direct the remainder of the intubation strategy, including preoxygenation, medications, patient positioning, operator training, laryngoscope type, and video assistance. This is a realistic approach that would be generalizable to the typical ED experience. The power of this study was sufficient to then create subgroup analyses for each of these factors, and prove they were not confounders.
Weaknesses:
This study is primarily limited by its single center design and thus may not be generalizable to all Emergency Departments. This particular hospital had been using the bougie routinely prior to this study, which is uncommon. This may have led to overestimation of the bougie’s benefit. Further studies involving multi-centered trials are needed to affirm generalizability. Finally, this study by design could not be blinded, which could have led to biased results.
Take Home Points:
This was a single center randomized controlled trial of bougie vs ET tube + stylet for first-pass intubation
The bougie was significantly more effective in all patients, with or without difficult airway features
This study is potentially practice-changing and suggests the bougie should be used as a routine primary intubation device for all patients in the ED
Further studies including a multi-centered trial would be helpful to affirm generalizability
Expert Commentary
Thank you for the excellent review of this randomized trial of a bougie-first intubation strategy. I agree that this study is potentially practice-changing, with the important caveat that your initial mileage may vary due to the study setting of a single ED with an existing culture of utilizing the bougie. Still, the demonstrated 11% absolute difference in first-pass success among all-comers (including patients with and without difficult airway characteristics) is compelling.
Intuitively, routine use of the bougie should be a familiar concept to ED physicians. We regularly utilize Seldinger technique in the placement of various vascular access devices, and the bougie can be thought of as the Seldinger technique of the airway. Anecdotally, I feel that the primary benefits of the bougie are improved visualization of the glottic inlet and tactile feedback from tracheal clicks and holdup. Many of us will encounter airways that we do not initially perceive to be difficult based on anatomic features (e.g., non-obese, reassuring Mallampati) only to be perplexed by the visual appearance of the glottic inlet after blade placement (see Kovacs et al., 2017) or complete obscuring of the glottic inlet by rapidly re-accumulating blood or vomitus. In these scenarios, tactile feedback can be reassuring of proper tube placement.
Importantly, use of the bougie requires the operator to understand three key points: first, many novice users instinctively remove the intubating blade after the bougie is placed but prior to railroading the endotracheal (ET) tube over the bougie; this makes ET tube placement difficult but can be addressed by re-inserting the intubating blade (and confirming that the bougie remains in the correct position). Second, as the study authors point out, the bevel tip of the endotracheal tube can get caught on the arytenoids. This can be addressed by rotating the ET tube and re-attempting insertion. Finally, bougie placement can be difficult with hyper-angulated devices, such as the traditional GlideScope blade or the “D-Blade” for the C-MAC – hence the reason for excluding these devices in the trial. These hyper-angulated devices require the ET tube (and bougie) to navigate a hyper-acute angle for delivery, which is why they come with a special hyper-angulated metal stylet.
Finally, while I am an advocate of a bougie-first intubation strategy, I would emphasize that it is important not to become too infatuated with or dependent on a single airway technique. For example, a bougie cannot solve the dilemma of a small, restricted mouth that will not accommodate blade placement (e.g., advanced scleroderma), nor will it allow you to navigate an edematous tongue that occludes the entire oropharynx (e.g., severe angioedema). The best airway technicians are facile in a number of airway techniques, are always cognizant of the potential for their primary approach to be unsuccessful, and have a clear algorithm for how to respond to potential obstacles. This requires learning as many airway techniques as possible during your training (e.g. video, direct, LMA, bougie, fiber-optic).
References:
Kovacs G, Duggan LV, Brindley PG. Glottic Impersonation. Can J Anaesth. 2017 Mar;64(3):320. PMID 28028675.

Howard S. Kim, MD MS
Assistant Professor
Department of Emergency Medicine
Northwestern University Feinberg School of Medicine
How To Cite This Post
[Peer-Reviewed, Web Publication] Randolph A, Colton K. (2019, Nov 25). Bougie Journal Club. [NUEM Blog. Expert Commentary by Kim H]. Retrieved from http://www.nuemblog.com/blog/bougie.
Other Posts You May Enjoy
Featured









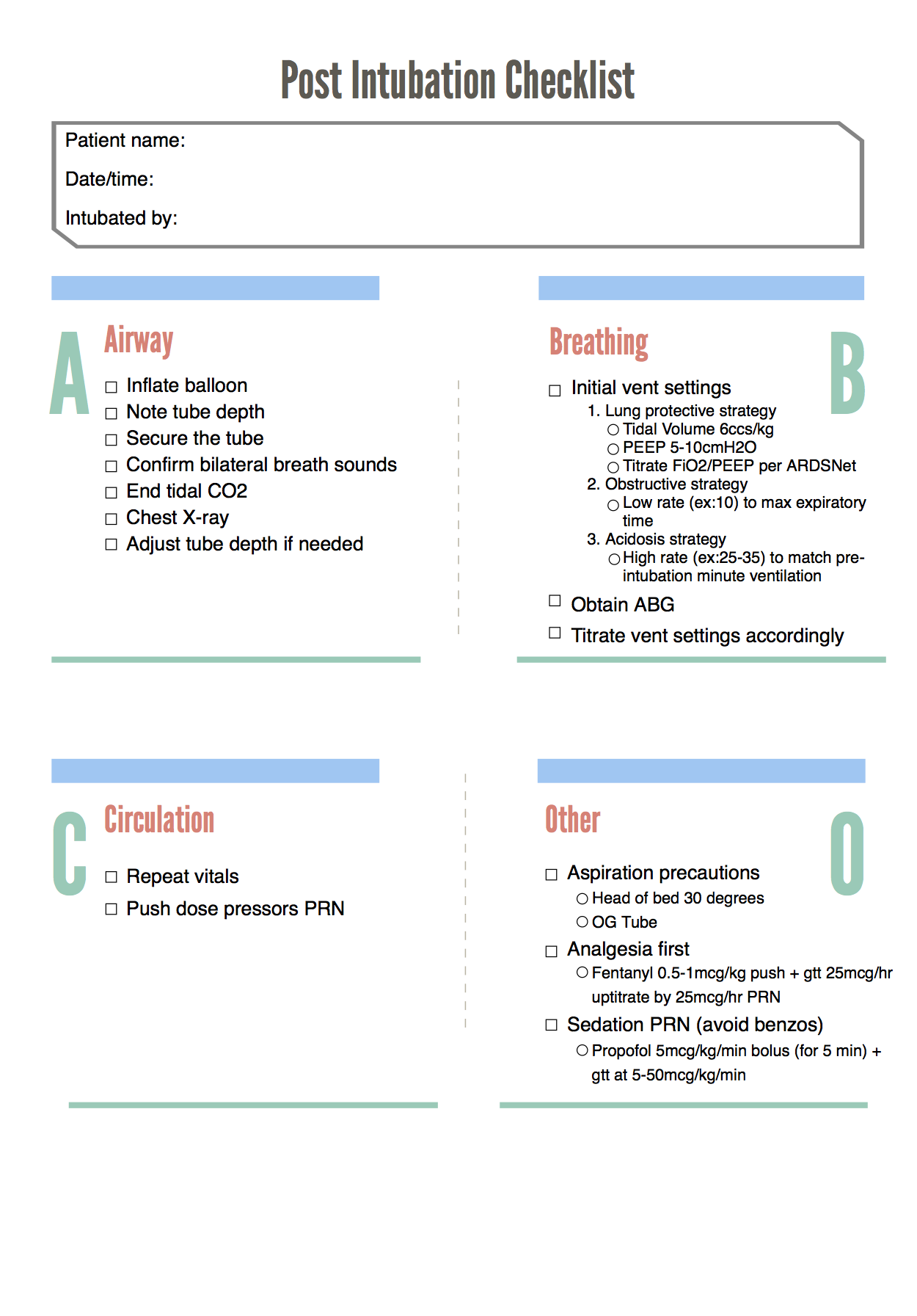
Post-Intubation Checklist

Written by: Andra Farcas, MD (NUEM PGY-2) Edited by: Paul Trinquero, MD (NUEM PGY-4) Expert commentary by: Andrew Pirotte, MD
Developing a Post-Intubation Checklist
Multiple studies have shown checklists in medicine can be beneficial. They have been used to reduce rates of catheter-related blood stream infections and ventilator associated pneumonias and to improve team performance in various settings.
In the ED setting, a peri-intubation checklist for trauma patients resulted in more use of rapid sequence intubation and a trend towards improvement in post-intubation sedation rates.[1] This checklist included meds for pre-intubation (pre-treatment, induction, paralytics) and information about which intubation device was used but had only one line for post-intubation medications and did not include other post-intubation safety measures.
One of the few studies that we could find specifically focused on a post-intubation checklist was a MICU study by McConnell, et al. They looked at the proportion of patients who had an ABG drawn within 60 minutes of mechanical ventilation initiation, as well as rates of respiratory acidosis and acidemia. They found that after initiating a post-intubation checklist and timeout, the rates of ABGs increased, which led to earlier recognition of inappropriate ventilation settings.
There are a lot of pre-intubation checklists available for public use. For example, a great podcast/blogpost by Scott Weingart on the topic was developed into a checklist by Jeffrey Siegler and Christ Huntley. Their versions can be found at https://emcrit.org/emcrit/post-intubation-package/.
Our goal was to design a checklist specifically for the post-intubation setting that could potentially be implemented in our emergency department. We took ideas from aforementioned studies and existing checklists, as well as personal experience. In addition to covering a broad array of post-intubation tasks, we wanted to focus especially on post-intubation sedation and initial vent settings. In regards to these important tasks, what we do in the ED matters. Not only are the first few hours a critical period in the course of illness, but there is significant downstream momentum associated with choices made in the Emergency Department.
The SPICE trial showed a link between deep early sedation and prolonged ventilation and increased mortality.[6] Conversely, an analgesia only, no-sedation approach has been shown to reduce time on the ventilator.[7] Consequently, we advocate for an analgesia-first approach. Fentanyl is a commonly used opioid for this purpose because of its rapid onset and short half-life. An easy starting point is a 0.5 - 1mcg/kg fentanyl push, followed by a drip starting at 25mcg/hr and uptitrated by 25mcg every 15-30 minutes (concurrent with another bolus as needed to control pain).
If pain is under control and additional sedation is needed, there are many options. Propofol is commonly used and is easily titratable. Start with a bolus of 5 mcg/kg/min (for 5 min) and start the drip at 5 to 10 mcg/kg/min, increasing by 5-10mcg/kg/min intervals every 5 min as needed (usual range 5-50mcg/kg/min). In the case of hypotension precluding the use of propofol, consider ketamine. Try to avoid benzodiazepines as these have been shown to increase risk of delirium.
Similarly, the initial vent settings that we chose in the ED matter and they can affect duration of ventilation, ICU length of stay, hospital length of stay, and other patient-oriented outcomes.[2] Not all illnesses requiring intubation and mechanical ventilation are the same and consequently vent-settings are not a one size fits all selection. Try to tailor settings to the individual patient and illness and choose one of the following broad strategies[9]:
Lung Protective Strategy (ARDS, lung injury, default for most patients): goal is to minimize additional injury via volutrauma or barotrauma. Set the tidal volume at 6-8cc per kg (of ideal body weight). Soon after intubation, drop Fio2 to 30% and PEEP to 5cm then titrate according to ARDSNet strategy for goal oxygen saturation 88-95%.
Obstructive Strategy (asthma or COPD): goal is to minimize air trapping by maximizing expiration time. Hence, set a low rate (perhaps 10) which will minimize I:E ratio (perhaps 1:4). Tidal volume can be standard 8cc/kg. This strategy may require permissive hypercapnea.
Severe acidosis (DKA, severe sepsis, etc.): Goal is to mimic the pre-intubation minute ventilation. Set the respiratory rate to match pre-intubation rate (usually at least 25-30).
Below is our designed post-intubation checklist:
Expert Commentary
This column highlights the need for optimized post-intubation management. This process requires attention to detail and patient needs. Effective management not only involves delivery of adequate analgesia and sedation, but also efficient titration of the ventilator. Each of these aspects of post-intubation management can be multi-faceted and challenging. To assist with these processes and to simplify tasks, a checklist can be of great value.
Checklists can help create a stepwise clinical approach and trigger timely delivery of individual tasks. Checklists can also help prevent omission of vital steps. A task as simple as a chest X-ray to confirm endotracheal tube placement and positioning can be overlooked in an emergent situation. The checklist provided in the review provides a simple, direct pathway to assist with post-intubation management, and avoid task omission. In addition, this checklist can help emphasize strategies in the post-intubation period. For example, the use of an “analgesic first” pathway for patient comfort following intubation.
As stated in the blog post, evidence now suggests “analgesic first” pathways improve patient outcomes. The clinician should strive to enhance analgesia prior to escalating sedation. Sedation has its role in post-intubation management, but should be employed only if escalated analgesic efforts fail. “Analgesic first” pathways decrease ICU length of stay, decrease complications, and improve outcomes. In addition to managing patient comfort, the clinician must also focus on optimizing ventilation and oxygenation.
Successful ventilator management requires attention to detail and the clinical scenario. Every patient has different ventilation and oxygenation needs. In addition to frequently reevaluating the patient clinically, a common and effective strategy for optimizing a ventilated patient is use of frequent blood gas measurement. Titration of ventilation and oxygenation can be aided greatly with serial blood gas monitoring. The use of blood gas data can also guide the provider utilizing a specific ventilation strategy (eg Lung-protective strategy). Common problems in early post-intubation management include excessive oxygen delivery and hypoventilation. Both of these can be identified by blood gas sampling. Once optimal ventilation and oxygenation is achieved, the clinician can proceed with further diagnostic and stabilization pathways.
Within the airway community, much focus is placed on optimized laryngoscopy and endotracheal tube delivery, no desaturation during intubation, interesting new equipment, etc. However, managing an airway does not conclude with delivery of the endotracheal tube. All clinicians managing airways would benefit greatly from accompanying this enthusiasm for intubation with focused and detailed care (often supplemented by checklists) in the post-intubation period.
Special thanks to Dr. Jordan Kaylor and Dr. Matthew Pirotte

Andrew Pirotte, MD
Department of Emergency Medicine, University of Kansas Hospital
Clinical Assistant Professor, University of Kansas Medical Center
How To Cite This Post
[Peer-Reviewed, Web Publication] Farcas A, Trinquero P (2019, February 11). Post-Intubation Checklist [NUEM Blog. Expert Commentary by Pirotte A]. Retrieved from http://www.nuemblog.com/blog/post-intubation
Other Posts You Might Enjoy









References
Conroy, M.J., Weingart, G.S., Carlson, J.N. Impact of checklists on peri-intubation care in ED trauma patients. American Journal of Emergency Medicine, 2014; 32:541-544.
Fuller, B.M., Ferguson, I.T., Mohr, N.M., Drewery, A.M., Palmer, C., Wessman, B.T. et al. Lung-Protective Ventilation Initiated in the Emergency Department (LOV-ED): A Quasi-Experimental, Before-After Trial. Annals of Emergency Medicine, 2017; 70(3):406-418.
Guthrie, K., Rippey, J. Emergency Department Post-Intubation Checklist. Agency for Clinical Innovation, 2013. https://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0003/273792/emergency-department-post-intubation-checklist-charles-gairdner.pdf. Accessed May 26, 2018.
McConnell, R.A., Kerlin, M.P., Schweickert, W.D., Ahmad, F., Patel, M.S., Fuchs, B.D. Using a Post-Intubation Checklist and Time Out to Expedite Mechanical Ventilation Monitoring: Observational study of a Quality Improvement Intervention. Respiratory Care, 2016; 61(7):902-912.
Nickson, C. Post-intubation care. Life In The Fast Lane, Jan 5 2013. https://lifeinthefastlane.com/ccc/post-intubation-care/. Accessed May 26, 2018.
Shehabi, Y., Bellomo, R., Reade, M., Bailey, M., Bass, F., Howe, B. et al. Early Intensive Care Sedation Predicts Long-Term Mortality in Ventilated Critically Ill Patients. American Journal of Respiratory and Critical Care Medicine, 2012; 186(8):724-731.
Strøm, T., Martinussen, T., Toft, P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. The Lancet, 2010; 375:475-480
Weingart, S. Podcast 84 – The Post-Intubation Package. EMCrit RACC, Oct 16 2012. https://emcrit.org/emcrit/post-intubation-package/. Accessed May 26, 2018.
Weingart, S. Managing Initial Mechanical Ventilation in the Emergency Department. Annals Of Emergency Medicine, 2016; 68(5):614-61
Intubation Positioning: Beyond Sniffing
Written by: Katie Colton, MD (NUEM PGY-4) Edited by: Charles Caffrey, MD (NUEM Alum ‘18) Expert commentary by: Andrew Pirotte, MD
The patient
On a recent Thursday night in a single-attending ED, we received a call that a patient was several minutes out with respiratory distress. He had been enjoying his routine post-dinner cocaine insufflation and became dyspneic, per bystanders. We could hear yelling in the back of the ambulance and EMS reported that they were only able to get an oxygen saturation, which was about 70%.
The scene
Two minutes later, EMS rushed in with a patient who looked to be in his mid-50s who was clearly struggling to breathe; it required 6 people to transfer him to our cart. He was altered, hypoxic, approximately 500 pounds, and needing an airway in the near future. While there are many considerations for the difficult airway, what are particular positioning options that may increase the chances of success in this patient?
“Positioning is 90% of the battle”
Beyond the technical difficulties posed by the morbidly obese patient, there are physiologic differences that complicate their oxygenation and ventilation. Due to the weight of the chest and larger abdomen they will have a decreased functional residual capacity and total lung capacity. Supine position can complicate pre-oxygenation, endotracheal intubation (ETI), and cause hypotension in these patients.
Many providers are still trained almost entirely in ETI with a supine patient, but there is growing evidence that a head-up position can improve pre-oxygenation and facilitate ETI.
Some authors advocate for an aggressive ramped position, using either a pre-formed foam ramp or a stack of pillows or blankets, like in the pictures below. I would argue that unless you have a stack of pillows at the ready and a number of spare hands this technique may be difficult in the less-controlled setting.

(Simoni 2005)

So then what?
Newer studies – and anecdotal experience - are showing good results with upright intubation through simple manipulation of the head of the bed. One example of this is the back-up head-elevated position as seen below[2]. First, by brief placement of the patient into Trendelenburg, the patient is brought all the way to the top of the bed (1 in image), and then the back of the bed is ramped up to at least 30 degrees above the horizontal (2 in image), with the head placed into the “sniffing” position with a towel roll (3 in image).[2] In their retrospective analysis, Khandelwal et al. found a lower rate of intubation-related complications as compared to a supine cohort, 9.3% vs 22.6%.[2]
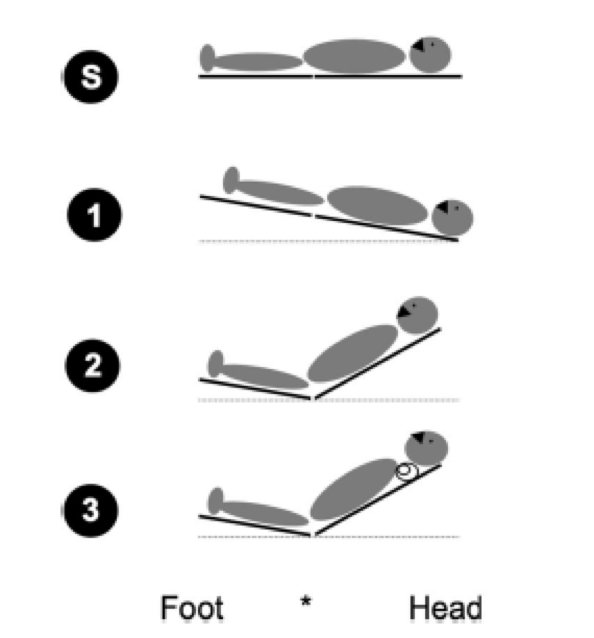
(Khandewal 2016)
How to place the patient in the advised back-up, head-elevated position.
A team from IU showed improved intubation success with head of bed elevation in both a simulated [4] and ED setting [3]. This approach allows the patient to be positioned during preoxygenation. Redundant tissue falls away from the face and chest, improving the patients ability to breathe for themselves and the ease of BVM, if needed. Khandelwal et al found lower risk of aspiration and esophageal tube placement. For every 5 degree increase in head of bed angulation above the horizontal, Turner et al found increased likelihood of first pass success with ETI.

(Turner 2017)
In short, consider using the bed to your advantage in these difficult patients. It takes time to overcome habits but there is good evidence for changing up your positioning plan.
Case Conclusion
The patient’s head of the bed was ramped up to 45 degrees. Utilizing rapid sequence intubation, the resident took one look with a size 4 Macintosh acquiring a Grade II view, and was able to place an 8-0 tube. A follow-up chest x-ray showed appropriate placement and frank pulmonary edema. The patient was treated for pulmonary edema and admitted to the ICU.
Expert Commentary
As with all clinical excellence, the devil is in the details. Skillful airway management requires attention to detail, notably patient positioning. This case and review serve as a reminder that close attention to setup and positioning can help enhance successful airway management.
Positioning is critical to airway success. Particularly in the setting of higher body-mass index patients, optimized positioning is a critical step to safe and successful airway management. As suggested by the review, simply placing the patient in supine positioning is not optimal and should be avoided if possible. Improved positioning can be achieved in several ways, but often the most straight-forward is by raising the head of the bed, or stacking towels and pillows. This position is often referred to as the “sniffing” position.
The sniffing position refers to bringing the sternal notch and the ear into the same plain (see blog post image). This positioning not only improves ergonomics for the clinician, but provides enhanced laryngoscopy and endotracheal tube delivery success. In addition, sniffing positioning compliments and enhances other airway optimization strategies.
One significant benefit of the sniffing position is preventing collapse of soft tissue and occlusion of the airway. The relief of redundant tissue with the sniffing position likely improves high-quality mask ventilation, as the tissue collapse into the posterior oropharynx is less prominent. Physiological benefits of sniffing position also include decreased lung atelectasis and improved delivery of oxygen during airway preparation. Considering these points, utilization of the sniffing position (rather than supine positioning), vitally strengthens the airway management pathway.
Positioning remains crucial to optimized airway delivery. The sniffing position does not require expensive equipment or great skill; it is a straight-forward, useful, and impactful strategy to enhance airway management. As emergency airway management continues to evolve, much focus has been on enhancing laryngoscopy. In addition, there have been great strides in technology and monitoring equipment. But even with the best equipment and technology, simple strategies such as optimizing positioning can lead to high-yield results.
Special thanks to Dr. Jordan Kaylor and Dr. Matthew Pirotte

Andrew Pirotte, MD
Department of Emergency Medicine, University of Kansas Hospital
Clinical Assistant Professor, University of Kansas Medical Center
How to Cite This Post
[Peer-Reviewed, Web Publication] Colton K, Caffrey C (2019, February 4). Intubation Positioning: Beyond Sniffing [NUEM Blog. Expert Commentary by Pirotte A]. Retrieved from http://www.nuemblog.com/blog/intubation-positioning.
Other Posts You May Enjoy
Resources
RF Simoni et al. Tracheal Intubation of Morbidly Obese Patients: A Useful Device. Brazilian Journal of Anesthesiology, 2005; 55: 2: 256-260
N Khandelwal et al. Head-Elevated Patient Positioning Decreases Complications of Emergent Tracheal Intubation in the Ward and Intensive Care Unit. Anesth Analg. 2016 Apr;122(4):1101-7.
Turner JS et al. Feasibility of upright patient positioning and intubation success rates at two academic emergency departments. Am J Emerg Med. 2017 Feb 5. pii: S0735-6757(17)30100-6.
Turner JS et al. Cross-over study of novice intubators performing endotracheal intubation in an upright versus supine position. Intern Emerg Med. 2016 Jun 14.